You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cancer PathologyDocument7 pagesCancer PathologyRidha Surya NugrahaNo ratings yet
- Chronic Complications Diabetes - Acta Med Indones - Edit 8 Apr 14Document9 pagesChronic Complications Diabetes - Acta Med Indones - Edit 8 Apr 14Ridha Surya Nugraha100% (1)
- Cancer JournalDocument9 pagesCancer JournalRidha Surya NugrahaNo ratings yet
- MindMapper Tutorial PDFDocument1 pageMindMapper Tutorial PDFRidha Surya NugrahaNo ratings yet
- Basal Ganglia & Degenerative DisordersDocument46 pagesBasal Ganglia & Degenerative DisordersRidha Surya NugrahaNo ratings yet
- Cancer Malignancy TumorDocument6 pagesCancer Malignancy TumorRidha Surya NugrahaNo ratings yet
- Bangs atDocument1 pageBangs atRidha Surya NugrahaNo ratings yet
- Link Donlot FilmDocument1 pageLink Donlot FilmRidha Surya NugrahaNo ratings yet
- Cancer JournalDocument9 pagesCancer JournalRidha Surya NugrahaNo ratings yet
- Noise - Induced Hejaring Loss. (DR - Khayria) - 2mlkmlkmDocument13 pagesNoise - Induced Hejaring Loss. (DR - Khayria) - 2mlkmlkmRidha Surya NugrahaNo ratings yet
- Clinical of StrokeDocument31 pagesClinical of StrokeIlham riandaNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaRidha Surya NugrahaNo ratings yet
- Set Aaaaaaaaaaaa NNNDocument1 pageSet Aaaaaaaaaaaa NNNRidha Surya NugrahaNo ratings yet
- A A A AaaaaaaaaaaaaaaDocument1 pageA A A AaaaaaaaaaaaaaaRidha Surya NugrahaNo ratings yet
- Original Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodDocument6 pagesOriginal Article: Clinical and Laboratory Features of Typhoid Fever in ChildhoodRidha Surya NugrahaNo ratings yet
- 2008 SNAREmediated Membrane FusionDocument7 pages2008 SNAREmediated Membrane FusionRidha Surya NugrahaNo ratings yet
- 2008 Synaptic Vesicle FusionDocument10 pages2008 Synaptic Vesicle FusionRidha Surya NugrahaNo ratings yet
- Anemia Def FeDocument1 pageAnemia Def FeRidha Surya NugrahaNo ratings yet
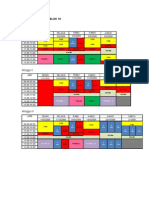
- Matriks Kegiatan Blok 10Document2 pagesMatriks Kegiatan Blok 10Ridha Surya NugrahaNo ratings yet
- 2007 TAG SynapticDocument5 pages2007 TAG SynapticRidha Surya NugrahaNo ratings yet
- RAV Nonproliferative Diabetic Retinopathy NPDRDocument1 pageRAV Nonproliferative Diabetic Retinopathy NPDRRidha Surya NugrahaNo ratings yet
- RAV Nonproliferative Diabetic Retinopathy NPDRDocument1 pageRAV Nonproliferative Diabetic Retinopathy NPDRRidha Surya NugrahaNo ratings yet
- Nej Me 1000091Document3 pagesNej Me 1000091Ridha Surya NugrahaNo ratings yet
- OijijlllllDocument1 pageOijijlllllRidha Surya NugrahaNo ratings yet
- Speedy Instal at IonDocument1 pageSpeedy Instal at IonRidha Surya NugrahaNo ratings yet
- Sdasldmk MCDMFL DSFDocument1 pageSdasldmk MCDMFL DSFRidha Surya NugrahaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Stable Bleaching PowderDocument1 pageStable Bleaching PowderAbhishek SharmaNo ratings yet
- Case Presentation PBL 12 (Bipolar Disorder)Document65 pagesCase Presentation PBL 12 (Bipolar Disorder)Rhomizal Mazali83% (6)
- Abdomenul AcutDocument5 pagesAbdomenul Acutcristina ovidenieNo ratings yet
- Reading Activity ANDREA ALMENDARES 2DO PARCIALDocument2 pagesReading Activity ANDREA ALMENDARES 2DO PARCIALAndrea Almendares Vasquez0% (1)
- 1.1 Plumbing History and Terminologies - Building Utilities 1 (Course Materials)Document13 pages1.1 Plumbing History and Terminologies - Building Utilities 1 (Course Materials)Princessdy CocadizNo ratings yet
- Cushing's Syndrome, Addison's Disease and Hyperparathyroidism.Document29 pagesCushing's Syndrome, Addison's Disease and Hyperparathyroidism.pranjl100% (1)
- Ati Communication NR 341 PDFDocument3 pagesAti Communication NR 341 PDFmp1757No ratings yet
- An Interactive 3D Acupressure Model For Self TreatDocument10 pagesAn Interactive 3D Acupressure Model For Self TreatJovana DragojlovicNo ratings yet
- Clinical QigongDocument5 pagesClinical QigongFlorin Iacob100% (1)
- Theory and Practice of Addiction Counseling I1686Document16 pagesTheory and Practice of Addiction Counseling I1686pollomaximus 444No ratings yet
- NPI Reflects Spring 2013Document12 pagesNPI Reflects Spring 2013npinashvilleNo ratings yet
- NCP - Acute PainDocument3 pagesNCP - Acute PainRoxanne NavarroNo ratings yet
- Review Shows EGb 761 Optimizes Standards of Life For Tinnitus PatientsDocument2 pagesReview Shows EGb 761 Optimizes Standards of Life For Tinnitus PatientsTotoDodongGusNo ratings yet
- Awake Craniotomy and Excision of A Diffuse Low Grade Glioma in A Multilingual PatientDocument7 pagesAwake Craniotomy and Excision of A Diffuse Low Grade Glioma in A Multilingual PatientNatalyNo ratings yet
- Handbook: For Clinical Management of DengueDocument124 pagesHandbook: For Clinical Management of DengueraattaiNo ratings yet
- Is An Ancient Disease That Causes Permanent Physical Disability AmongDocument6 pagesIs An Ancient Disease That Causes Permanent Physical Disability Amongkian5No ratings yet
- 1.7 Right Person, Right Place, Right Time PDFDocument3 pages1.7 Right Person, Right Place, Right Time PDFKaren Osorio GilardiNo ratings yet
- The FRCPath Exam - Paul BennettDocument130 pagesThe FRCPath Exam - Paul BennettVictor ChanNo ratings yet
- Vriddhi KshayaDocument37 pagesVriddhi KshayaVenkatesan VidhyaNo ratings yet
- Modern Trends in Hypnosis Ed by David Waxman & Prem C Misra & Michael Gibson & M Anthony Basker (1985)Document404 pagesModern Trends in Hypnosis Ed by David Waxman & Prem C Misra & Michael Gibson & M Anthony Basker (1985)marcinlesniewicz100% (4)
- SCAI Shock Classification DeckDocument22 pagesSCAI Shock Classification DeckJimmy JimmyNo ratings yet
- The Placebo EffectDocument2 pagesThe Placebo EffectMeshack RutoNo ratings yet
- Tutorial Assignment Week 14 With AnswerDocument4 pagesTutorial Assignment Week 14 With AnswerCik Wynn100% (1)
- Lifewater LatrineDesignandConstruction ManualDocument270 pagesLifewater LatrineDesignandConstruction ManualDelovan CheikhoNo ratings yet
- Hovenia Dulcis - Scientific Review On Usage, Dosage, Side Effects - ExamineDocument5 pagesHovenia Dulcis - Scientific Review On Usage, Dosage, Side Effects - Examineozman blooriNo ratings yet
- Current Directions in ADHD and Its TreatmentDocument314 pagesCurrent Directions in ADHD and Its TreatmentSofía Lecter100% (1)
- Cold ApplicationDocument2 pagesCold ApplicationNazire Luis Colita YandugNo ratings yet
- Acupuncture IVFDocument10 pagesAcupuncture IVFWolfgang Rb100% (1)
- Curosurf 120mg / Vial Endotracheopulmonary Instillation Suspension Curosurf 240mg / Vial Endotracheopulmonary Instillation SuspensionDocument2 pagesCurosurf 120mg / Vial Endotracheopulmonary Instillation Suspension Curosurf 240mg / Vial Endotracheopulmonary Instillation SuspensionHerlinsye PurimahuaNo ratings yet
- Tintin Cooking Beans and LegumesDocument3 pagesTintin Cooking Beans and LegumesBiZayangAmaZonaNo ratings yet