You might also like
- Conservative Management of Ectopic Pregnancy: A Provincial Hospital Case Series of Medically Managed Ectopic PregnanciesDocument5 pagesConservative Management of Ectopic Pregnancy: A Provincial Hospital Case Series of Medically Managed Ectopic PregnanciesSandy JusiNo ratings yet
- Endometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDocument4 pagesEndometrial Adenocarcinoma and Polycystic Ovary Syndrome: Risk Factors, Management, and PrognosisDikie MustofadijayaNo ratings yet
- Post Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsDocument5 pagesPost Hysteroscopic Progesterone Hormone Therapy in The Treatment of Endometrial PolypsherryNo ratings yet
- What Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?Document6 pagesWhat Is The Recurrence Rate of Postmenopausal Bleeding in Women Who Have A Thin Endometrium During A First Episode of Postmenopausal Bleeding?dwiagusyuliantoNo ratings yet
- Validity of Hysteroscopy in Detection of Uterine Cavity Abnormalities in Women With Recurrent Pregnancy LossDocument5 pagesValidity of Hysteroscopy in Detection of Uterine Cavity Abnormalities in Women With Recurrent Pregnancy LossPeertechz Publications Inc.No ratings yet
- Progestogen TreatmentDocument6 pagesProgestogen TreatmentIndah HaneNo ratings yet
- Ectopic Pregnancy and Its Effect On Future Fertility: Original StudiesDocument0 pagesEctopic Pregnancy and Its Effect On Future Fertility: Original StudiesnajmulNo ratings yet
- Abnormal Uterine Bleeding in A 39 Year OldDocument16 pagesAbnormal Uterine Bleeding in A 39 Year OldEliana GerzonNo ratings yet
- Clinical Case 53-Endometrial CarcinomaDocument4 pagesClinical Case 53-Endometrial Carcinomaselina kalenderNo ratings yet
- Article - Infertility Endometriosis PDFDocument5 pagesArticle - Infertility Endometriosis PDFFertility Talks Dr.Tabassum KhanNo ratings yet
- Free Paper Abstract BookDocument1,047 pagesFree Paper Abstract Bookkukadiya100% (1)
- Case 7 For TutorDocument7 pagesCase 7 For TutorwijiantotepasNo ratings yet
- 1 Sttri 3Document6 pages1 Sttri 3parkfishyNo ratings yet
- Surgical Outcome of Genito Urinary Fistula - RayazDocument3 pagesSurgical Outcome of Genito Urinary Fistula - RayazRiaz Ahmed ChaudhryNo ratings yet
- Comparison of Laparoscopy and Laparotomy in The Surgical Management of Ectopic PregnancyDocument5 pagesComparison of Laparoscopy and Laparotomy in The Surgical Management of Ectopic PregnancyFitri Maya AnggrainiNo ratings yet
- Endometrial Hyperplasia - Gyn ReviewDocument18 pagesEndometrial Hyperplasia - Gyn ReviewFedrik Monte Kristo LimbongNo ratings yet
- Adenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFDocument5 pagesAdenomyosis Excision Followed by Successful Live Birth After Three Consecutive IVFPyuzz RemakeNo ratings yet
- Fard Et Al., 2012Document6 pagesFard Et Al., 2012Jonathan LucisNo ratings yet
- Van Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournDocument5 pagesVan Wyk Grumbach Syndrome The Importance of Thyroi 2024 International JournRonald QuezadaNo ratings yet
- NbibDocument3 pagesNbibririndianpratiwisakinahNo ratings yet
- Sumabong NCM109 JOURNALREADINGDocument6 pagesSumabong NCM109 JOURNALREADINGMark VincentNo ratings yet
- Ectopic Pregnancy Risk Factors, Clinical Presentation and ManagementDocument6 pagesEctopic Pregnancy Risk Factors, Clinical Presentation and ManagementRizka AdiNo ratings yet
- Benign Breast Disease: Douglas J. Marchant, MDDocument20 pagesBenign Breast Disease: Douglas J. Marchant, MDchristel chadidNo ratings yet
- Presentation For Case StudyDocument36 pagesPresentation For Case Studybeng51264No ratings yet
- Somc 2019 - AbtractDocument1 pageSomc 2019 - Abtractmohammad abdulNo ratings yet
- Pretreatment of Leiomyoma With GNRH Agonists/Antagonists B of Any ValueDocument5 pagesPretreatment of Leiomyoma With GNRH Agonists/Antagonists B of Any ValueAdi TriNo ratings yet
- Management of Miscarriage: A Randomized Controlled Trial of Expectant Management Versus Surgical EvacuationDocument6 pagesManagement of Miscarriage: A Randomized Controlled Trial of Expectant Management Versus Surgical Evacuationjuçara bittemcurtNo ratings yet
- Quality of Life After Hysterectomy and UterusDocument4 pagesQuality of Life After Hysterectomy and UterusIvan Matthew SuperioNo ratings yet
- Omj D 09 00101Document6 pagesOmj D 09 00101DewinsNo ratings yet
- Reproductive Surgery: Laparoscopic Excision of Endometriosis: A Randomized, Placebo-Controlled TrialDocument7 pagesReproductive Surgery: Laparoscopic Excision of Endometriosis: A Randomized, Placebo-Controlled TrialAnonymous YyLSRdNo ratings yet
- 11.CaseReport3 V4I4 PDFDocument3 pages11.CaseReport3 V4I4 PDFSUSPANo ratings yet
- Management of Anembryonic Pregnancy Loss: An Observational StudyDocument6 pagesManagement of Anembryonic Pregnancy Loss: An Observational StudyAnonymous ORleRrNo ratings yet
- Palagiano 2004Document11 pagesPalagiano 2004ShirleyNo ratings yet
- Abnormal Uterine BleedingDocument22 pagesAbnormal Uterine BleedingAde JuandaNo ratings yet
- Vesicovaginal FistulaDocument6 pagesVesicovaginal FistulaMaiza TusiminNo ratings yet
- General Gynaecology:, Leo Francis AquilizanDocument15 pagesGeneral Gynaecology:, Leo Francis AquilizanesjayemNo ratings yet
- Art 3A10.1007 2Fs00192 017 3304 9Document6 pagesArt 3A10.1007 2Fs00192 017 3304 9Khaleed KandaraNo ratings yet
- Scar Ectopic Case ReportDocument6 pagesScar Ectopic Case ReportMominah MayamNo ratings yet
- Green Journal ROMADocument9 pagesGreen Journal ROMAinvestorpatentNo ratings yet
- Mifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisDocument6 pagesMifepristone and Misoprostol For Early Pregnancy Failure: A Cohort AnalysisBobby SetiawanNo ratings yet
- Ultrasonics Sonochemistry: Jae-Seong Lee, Gi-Youn Hong, Byung-Joon Park, Tea-Eung KimDocument6 pagesUltrasonics Sonochemistry: Jae-Seong Lee, Gi-Youn Hong, Byung-Joon Park, Tea-Eung KimTantonio Tri PutraNo ratings yet
- Afhs0801 0044 2Document6 pagesAfhs0801 0044 2Noval FarlanNo ratings yet
- Health-Related Quality of Life in Adult MediterranDocument21 pagesHealth-Related Quality of Life in Adult MediterrancxksvhszsvNo ratings yet
- Ovarian TorsionDocument24 pagesOvarian Torsionantidius johnNo ratings yet
- Endometrial Adenocarcinoma A Tahbso CaseDocument78 pagesEndometrial Adenocarcinoma A Tahbso CaseJohn Mark Obrero100% (1)
- Borderline Mucinous Ovarian Tumor Presenting As Pseudo Meigs SyndromeDocument4 pagesBorderline Mucinous Ovarian Tumor Presenting As Pseudo Meigs SyndromeJulie MayNo ratings yet
- Sangrado Uterino en UrgenciaDocument13 pagesSangrado Uterino en UrgenciaVictoria Oliva ZúñigaNo ratings yet
- University of Santo TomasDocument28 pagesUniversity of Santo TomasLyndon SayongNo ratings yet
- 11abnormal Uterine BleedingDocument32 pages11abnormal Uterine BleedingAkinbani MoyosoreNo ratings yet
- Bakker 2012Document10 pagesBakker 2012ieoNo ratings yet
- First Trimester Bleeding and Pregnancy Outcomes: Case-Control StudyDocument4 pagesFirst Trimester Bleeding and Pregnancy Outcomes: Case-Control StudyClara Nur RamadhaniNo ratings yet
- Impact of Oligohydramnios On Maternal and PerinataDocument6 pagesImpact of Oligohydramnios On Maternal and PerinataDiana SchlittlerNo ratings yet
- Jurnal 1Document10 pagesJurnal 1Nia FebriyaniNo ratings yet
- Pelvic Pain in EndometriosisDocument7 pagesPelvic Pain in Endometriosism_tonydharmawanNo ratings yet
- 10.1007@s12325 020 01299 WDocument10 pages10.1007@s12325 020 01299 WBerry BancinNo ratings yet
- En Dome Trio 4Document7 pagesEn Dome Trio 4DONATA URBANINo ratings yet
- Our Experience With Adnexal Masses in The Pediatric Age Group and Review of LiteratureDocument6 pagesOur Experience With Adnexal Masses in The Pediatric Age Group and Review of LiteratureEdwin CalleNo ratings yet
- 16 Prolapse IndonesianDocument17 pages16 Prolapse IndonesianDwi MahendraNo ratings yet
- Jurnal - Postpartum Urinary RetentionDocument28 pagesJurnal - Postpartum Urinary RetentionBoyParadiseNo ratings yet
- Clinical CaseDocument10 pagesClinical CaseRoberto RamosNo ratings yet
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Case 3Document8 pagesCase 3Roberto RamosNo ratings yet
- Case 2 AlmostDocument8 pagesCase 2 AlmostRoberto RamosNo ratings yet
- Rhie Full OcrDocument120 pagesRhie Full OcrRoberto RamosNo ratings yet
- Universidad de Puerto Rico Mail - (No Subject)Document77 pagesUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosNo ratings yet
- Case 4Document8 pagesCase 4Roberto RamosNo ratings yet
- McCowan SGA RiskFactors BJOG 2010Document9 pagesMcCowan SGA RiskFactors BJOG 2010Roberto RamosNo ratings yet
- Long Case Presentation FINAL-33Document7 pagesLong Case Presentation FINAL-33Roberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Paciente 3Document80 pagesPaciente 3Roberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Radio ObGynDocument1 pageRadio ObGynRoberto RamosNo ratings yet
- Repaso ShelfDocument135 pagesRepaso ShelfRoberto RamosNo ratings yet
- Progress Note Osce - HIV (1) - 2Document1 pageProgress Note Osce - HIV (1) - 2Roberto RamosNo ratings yet
- SEPSIS Case 2014 - August-2Document45 pagesSEPSIS Case 2014 - August-2Roberto RamosNo ratings yet
- Final - Answers of Ekg QuizDocument46 pagesFinal - Answers of Ekg QuizRoberto RamosNo ratings yet
- "Repaso" Shelf OB - GYN 2 2Document9 pages"Repaso" Shelf OB - GYN 2 2Roberto RamosNo ratings yet
- Untitled Spreadsheet 2Document4 pagesUntitled Spreadsheet 2Roberto RamosNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
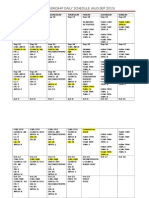
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Document3 pagesOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosNo ratings yet
- Health Maintenance Cases For Discussion-5Document4 pagesHealth Maintenance Cases For Discussion-5Roberto RamosNo ratings yet
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- Clinmed 19 3 261bDocument2 pagesClinmed 19 3 261bgevowo3277No ratings yet
- Hazard Identification and Prevention: (Ndlon-Osha)Document12 pagesHazard Identification and Prevention: (Ndlon-Osha)Eugine BalomagaNo ratings yet
- Prescription Pattern and Glycaemic Control Using Glycated Haemoglobin in Type 2 Diabetic Patients A Cross-Sectional SurveyDocument9 pagesPrescription Pattern and Glycaemic Control Using Glycated Haemoglobin in Type 2 Diabetic Patients A Cross-Sectional SurveyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cystic Fibrosis Patient PamphletDocument2 pagesCystic Fibrosis Patient PamphletfloapaaNo ratings yet
- Regulation of PhytophrameuticalDocument48 pagesRegulation of Phytophrameuticalmeghavathnaik100% (1)
- Drug Study Table OkDocument29 pagesDrug Study Table OkRifa'atul Mahmudah100% (1)
- NCP Klippel Trenaunay SyndromeDocument3 pagesNCP Klippel Trenaunay SyndromePaola Marie VenusNo ratings yet
- Immediate Newborn CareDocument1 pageImmediate Newborn CareClarissa GuifayaNo ratings yet
- Diabetes ProjectDocument12 pagesDiabetes ProjectRyan O'Neill50% (2)
- Fundamentals of Nursing Post Test Nov. 2016Document5 pagesFundamentals of Nursing Post Test Nov. 2016Jay Abasolo0% (1)
- Nurse Deployment Program NDP Examination NotesDocument44 pagesNurse Deployment Program NDP Examination NotesAngelo Quixote100% (1)
- Deep Impacted Mandibular Second MolarDocument4 pagesDeep Impacted Mandibular Second Molarkiara wardanaNo ratings yet
- Introduction To PharmacologyDocument11 pagesIntroduction To PharmacologyMaryam ElammaryNo ratings yet
- TCCC Quick Reference Guide 2017Document54 pagesTCCC Quick Reference Guide 2017https://www.t-medical.orgNo ratings yet
- Short CV SidartawanDocument2 pagesShort CV SidartawanHarry Margatama SaddhasagaraNo ratings yet
- WI-HSD-01 MALVAR Medical ConsultationDocument2 pagesWI-HSD-01 MALVAR Medical ConsultationVictor BaluyotNo ratings yet
- Damilola Olarewaju Lab 4Document5 pagesDamilola Olarewaju Lab 4api-535000853No ratings yet
- NCP: Diabetes Mellitus Prepregnancy/GestationalDocument11 pagesNCP: Diabetes Mellitus Prepregnancy/GestationalJavie85% (13)
- Sample Letter of Medical NecessityDocument4 pagesSample Letter of Medical NecessityGregory RussellNo ratings yet
- Ass AsDocument1 pageAss AsMukesh BishtNo ratings yet
- Original PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFDocument41 pagesOriginal PDF Complementary and Alternative Therapies For Nursing Practice 5th PDFpaul.shropshire768100% (37)
- Suven Life Sciences Secures Two (2) Product Patents in Australia and Canada (Company Update)Document2 pagesSuven Life Sciences Secures Two (2) Product Patents in Australia and Canada (Company Update)Shyam SunderNo ratings yet
- Facet Joint Pain-Advances in Patient Selection and TreatmentDocument16 pagesFacet Joint Pain-Advances in Patient Selection and TreatmentthiagoNo ratings yet
- CASE REPORT - Bronkopneumonia InggrisDocument39 pagesCASE REPORT - Bronkopneumonia InggrisGea AdindaNo ratings yet
- Asda Floss - Google SearchDocument1 pageAsda Floss - Google SearchMohammed Al-AminNo ratings yet
- Good BookDocument22 pagesGood BookWaqasAliNo ratings yet
- Sem1 Down SyndromeeeDocument5 pagesSem1 Down SyndromeeeRomina ReidNo ratings yet
- ICU Progress Note Template-RevisedDocument1 pageICU Progress Note Template-RevisedOlivia Michelle Vaughan67% (3)
- Infusion Set and Blood Transfusion SetDocument56 pagesInfusion Set and Blood Transfusion Setsaahil_goje1400No ratings yet
- Prosthetic Rehabilitation of A Maxillectomy Patient With A Titanium Closed Hollow Bulb Obturator Using Lost Wax Bolus Technique - A Case ReportDocument8 pagesProsthetic Rehabilitation of A Maxillectomy Patient With A Titanium Closed Hollow Bulb Obturator Using Lost Wax Bolus Technique - A Case ReportIJAR JOURNALNo ratings yet