You might also like
- POST-TEST Mock Written Diplomate ExaminationDocument62 pagesPOST-TEST Mock Written Diplomate ExaminationRem AlfelorNo ratings yet
- OB Williams Chap 2 Maternal AnatomyDocument7 pagesOB Williams Chap 2 Maternal AnatomyRem Alfelor0% (1)
- Chap 8 Prenatal CareDocument9 pagesChap 8 Prenatal CareRem AlfelorNo ratings yet
- OB Williams Chap 2 Maternal PhysiologyDocument9 pagesOB Williams Chap 2 Maternal PhysiologyRem Alfelor100% (2)
- Chapter 4 Maternal PhysiologyDocument12 pagesChapter 4 Maternal PhysiologyRem AlfelorNo ratings yet
- Chapter 2 Maternal AnatomyDocument9 pagesChapter 2 Maternal AnatomyRem Alfelor100% (2)
- Chapter 3 Congenital Genitourinary AbnormalitiesDocument4 pagesChapter 3 Congenital Genitourinary AbnormalitiesRem AlfelorNo ratings yet
- Psychiatric History and Mental Status ExaminationDocument6 pagesPsychiatric History and Mental Status ExaminationRem AlfelorNo ratings yet
- Case 01 - Maternal PhysiologyDocument5 pagesCase 01 - Maternal PhysiologyRem AlfelorNo ratings yet
- Retinoblastoma QuizDocument1 pageRetinoblastoma QuizRem AlfelorNo ratings yet
- Community Medicine Cavite ReportDocument46 pagesCommunity Medicine Cavite ReportRem AlfelorNo ratings yet
- Ent Case Report Acute Otitis Media Stage IIIDocument12 pagesEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- Generalities of Blood and Its ElementsDocument3 pagesGeneralities of Blood and Its ElementsRem AlfelorNo ratings yet
- Comprehensive Gynecology Uterine BleedingDocument7 pagesComprehensive Gynecology Uterine BleedingRem AlfelorNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Cengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test BankDocument26 pagesCengage Advantage Books Fundamentals of Business Law Excerpted Cases 3rd Edition Roger Leroy Miller Test Bankladonnaaidanm5s100% (28)
- Line CodingDocument27 pagesLine CodingshridonNo ratings yet
- Mechanical Components SectionDocument428 pagesMechanical Components Sectionxristo xristovNo ratings yet
- Maths Class Xii Sample Paper Test 02 For Board Exam 2023Document6 pagesMaths Class Xii Sample Paper Test 02 For Board Exam 2023Priyanshu KasanaNo ratings yet
- MEAMTA2-Assignment 2Document5 pagesMEAMTA2-Assignment 2pfukanisibuyi7No ratings yet
- Case Study Oil and Gas - PowerpointDocument8 pagesCase Study Oil and Gas - PowerpointYaxssNo ratings yet
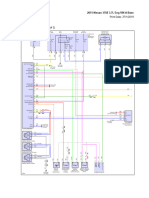
- 2015 Nissan 370Z 3.7L Eng VIN A BaseDocument69 pages2015 Nissan 370Z 3.7L Eng VIN A BaseData TécnicaNo ratings yet
- Bendable ConcreteDocument21 pagesBendable ConcreteJulia Sebastian0% (1)
- GirishDocument7 pagesGirishgsalunkhe241287No ratings yet
- Medical BiotechnologyDocument4 pagesMedical Biotechnologyعمر بن عليNo ratings yet
- FutbolistaDocument18 pagesFutbolistaKaren Osses50% (2)
- CON21 6th EditionDocument65 pagesCON21 6th EditionDavid WeeNo ratings yet
- Project Final PDFDocument98 pagesProject Final PDFNgonidzashe MhukaNo ratings yet
- Nonlinear Analysis and Optimal Design of Reinforced Concrete Plates and ShellsDocument17 pagesNonlinear Analysis and Optimal Design of Reinforced Concrete Plates and Shellsrodain najjarNo ratings yet
- Chapter Eight - Vapour Compression CycleDocument37 pagesChapter Eight - Vapour Compression Cyclealhusseny100% (1)
- How To Make FireworksDocument14 pagesHow To Make FireworksLeonardo BiancoNo ratings yet
- Hardie Reveal Panel Installation Instructions 1597005Document29 pagesHardie Reveal Panel Installation Instructions 1597005David TorskeNo ratings yet
- PEPSIDocument99 pagesPEPSIkingloiyaNo ratings yet
- 447.010 Screen Operating Manual v001Document67 pages447.010 Screen Operating Manual v001José CarlosNo ratings yet
- Da13 DDR N1 14000305 254 0Document3 pagesDa13 DDR N1 14000305 254 0Hamed NazariNo ratings yet
- Spread of Hinduism To South East Asia by Land and Maritime RoutesDocument36 pagesSpread of Hinduism To South East Asia by Land and Maritime RoutesUday DokrasNo ratings yet
- Morality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordDocument3 pagesMorality Speaks of A System of Behavior in Regards To Standards of Right or Wrong Behavior. The WordTHEO DOMINIC REQUERME SILVOSANo ratings yet
- Cryogenic Insulation TechnologyDocument61 pagesCryogenic Insulation Technologyeduard.turon100% (1)
- TM TC For NanosatelliteDocument4 pagesTM TC For NanosatelliteSreeja SujithNo ratings yet
- 4 TH Sem UG Osmoregulation in Aquatic VertebratesDocument6 pages4 TH Sem UG Osmoregulation in Aquatic VertebratesBasak ShreyaNo ratings yet
- Nelson Tables All in One PDFDocument618 pagesNelson Tables All in One PDFAmulya Ramakrishna100% (7)
- 365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusDocument10 pages365-M - City Bus Route & Timings, Bangalore (BMTC) Map, First & Last BusER Aditya DasNo ratings yet
- VK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualDocument76 pagesVK-53 (ВК-53) Erecting Cut-Out Switch: Maintenance ManualhaileNo ratings yet
- Zen Intro To Buddhism & Practice of ZazenDocument33 pagesZen Intro To Buddhism & Practice of ZazendudcomeonNo ratings yet
- Gurps Fallout HandgunsDocument1 pageGurps Fallout HandgunsAndrew Scott100% (1)