You might also like
- K Opiods For Pain BupDocument2 pagesK Opiods For Pain Bupandrew herringNo ratings yet
- Original Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve BlockDocument7 pagesOriginal Article: Serratus Plane Block: A Novel Ultrasound-Guided Thoracic Wall Nerve Blockandrew herringNo ratings yet
- Roux 2013Document7 pagesRoux 2013andrew herringNo ratings yet
- Highland Guidelines - LDK 2013-2-15Document3 pagesHighland Guidelines - LDK 2013-2-15andrew herringNo ratings yet
- Buprenorphine 2016-7-18Document1 pageBuprenorphine 2016-7-18andrew herringNo ratings yet
- Rib Fracture SerratusDocument3 pagesRib Fracture Serratusandrew herring100% (1)
- Intravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-OperatóriaDocument6 pagesIntravenous Lidocaine To Treat Postoperative Pain : Lidocaína Intravenosa No Tratamento Da Dor Pós-Operatóriaandrew herringNo ratings yet
- Rib Fracture W: PecsDocument8 pagesRib Fracture W: Pecsandrew herring100% (1)
- 3.2.16.highland Emergency Medicine Journal Club Methods.2Document2 pages3.2.16.highland Emergency Medicine Journal Club Methods.2andrew herringNo ratings yet
- Herring ED Intractable Abdominal pain-N+VDocument1 pageHerring ED Intractable Abdominal pain-N+Vandrew herringNo ratings yet
- Dex For Dental Pain & SwellingDocument7 pagesDex For Dental Pain & Swellingandrew herring100% (1)
- CVS Action Plan v2Document1 pageCVS Action Plan v2andrew herringNo ratings yet
- Nej MR A 1511480Document9 pagesNej MR A 1511480Tohari Masidi AminNo ratings yet
- Ultrasound-Guided Block of TheDocument6 pagesUltrasound-Guided Block of Theandrew herringNo ratings yet
- Ketamine As Rescue Treatment FDocument8 pagesKetamine As Rescue Treatment Fandrew herringNo ratings yet
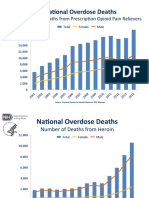
- OPR - Heroin DeathsDocument2 pagesOPR - Heroin Deathsandrew herringNo ratings yet
- Ultrasound Guided Interventional Procedures In.13Document14 pagesUltrasound Guided Interventional Procedures In.13andrew herring100% (1)
- Ultrasound Guided Interventional Procedures In.4Document13 pagesUltrasound Guided Interventional Procedures In.4andrew herringNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Agenda Bls-AclsDocument2 pagesAgenda Bls-AclsespegehNo ratings yet
- Intravenous AdmixturesDocument21 pagesIntravenous AdmixturesMichael AdjeiNo ratings yet
- MCQs Pharmacology - Series III-ADocument13 pagesMCQs Pharmacology - Series III-Asidharta_chatterjee100% (1)
- Craft Health Factsheet Ver1.4Document1 pageCraft Health Factsheet Ver1.4ravichandran0506No ratings yet
- Answers2ed OddDocument246 pagesAnswers2ed OddGaurav KamathNo ratings yet
- WHO Drug InformationDocument99 pagesWHO Drug Informationchromicutting100% (1)
- Sound Alike MedicationDocument1 pageSound Alike MedicationwaleedNo ratings yet
- Drug Card SennaDocument1 pageDrug Card SennaAdrianne Bazo100% (1)
- S2k Guidelines For The Treatment ofDocument12 pagesS2k Guidelines For The Treatment ofVinh ThếNo ratings yet
- Medication Adherence Scale PDFDocument13 pagesMedication Adherence Scale PDFRommel G. SantiagoNo ratings yet
- Pacu Tylenol PresentationDocument10 pagesPacu Tylenol PresentationStanford AnesthesiaNo ratings yet
- Med4Me BrochureDocument2 pagesMed4Me Brochureakhil4006No ratings yet
- Noninvasive VentilationDocument6 pagesNoninvasive VentilationEma MagfirahNo ratings yet
- List of Prescription AbbreviationsDocument5 pagesList of Prescription Abbreviationsrandatag100% (1)
- Qunoot Lakhani - Pharma Ospe FJDCDocument11 pagesQunoot Lakhani - Pharma Ospe FJDCNoor HaiderNo ratings yet
- Cupping Therapy in Brief by Shuaib SuriaDocument8 pagesCupping Therapy in Brief by Shuaib SuriaHussein A Bataineh100% (2)
- Páginas Desdepharmacotherapy Casebook 10th Ed.Document61 pagesPáginas Desdepharmacotherapy Casebook 10th Ed.Glo VsNo ratings yet
- Unit 4-InpatientDocument38 pagesUnit 4-InpatientSharmila LamisharNo ratings yet
- Acute Exacerbations of Asthma in Adults - Emergency Department and Inpatient Management (UPTODATE)Document32 pagesAcute Exacerbations of Asthma in Adults - Emergency Department and Inpatient Management (UPTODATE)Annie K.No ratings yet
- Introduction To BiopharmaceuticsDocument4 pagesIntroduction To BiopharmaceuticsIvymae TrillesNo ratings yet
- Transcribing Orders 2021 1Document51 pagesTranscribing Orders 2021 1blythe RiveroNo ratings yet
- Medication AdministrationDocument8 pagesMedication AdministrationMarku LeeNo ratings yet
- OmeprazoleDocument2 pagesOmeprazolephawphawphawNo ratings yet
- Therapeutic Drug MonitoringDocument10 pagesTherapeutic Drug MonitoringAnnie SethiNo ratings yet
- Mefenamic Acid Drug StudyDocument1 pageMefenamic Acid Drug Studymilkv70% (10)
- Management of GoutDocument6 pagesManagement of GoutSeanHong TanNo ratings yet
- FluconazoleDocument4 pagesFluconazoleeucaNo ratings yet
- Stok Qty - 05 Feb'22Document63 pagesStok Qty - 05 Feb'22Apotek C 8No ratings yet
- Yvonne Barnes-Holmes PBBT - Denmark Sep 2023 AarhusDocument2 pagesYvonne Barnes-Holmes PBBT - Denmark Sep 2023 AarhusGiancarlo ZPNo ratings yet
- Sedative HypnoticsDocument3 pagesSedative HypnoticsHemantNo ratings yet