You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- 14554522222Document5 pages14554522222igetisNo ratings yet
- 123Document7 pages123igetisNo ratings yet
- 33333339614856Document7 pages33333339614856igetisNo ratings yet
- DXGZSX 4446Document13 pagesDXGZSX 4446igetisNo ratings yet
- Document 2 summaryDocument5 pagesDocument 2 summaryigetisNo ratings yet
- Gys 54Document10 pagesGys 54igetisNo ratings yet
- OiuhygfDocument13 pagesOiuhygfigetisNo ratings yet
- 12655555Document13 pages12655555igetisNo ratings yet
- Gys 54Document10 pagesGys 54igetisNo ratings yet
- FDFBDocument6 pagesFDFBigetisNo ratings yet
- 215Document8 pages215igetisNo ratings yet
- Module 3Document20 pagesModule 3igetisNo ratings yet
- art3A10.11862Fs12884 015 0534 ZDocument13 pagesart3A10.11862Fs12884 015 0534 ZigetisNo ratings yet
- 456456Document4 pages456456igetisNo ratings yet
- 2368 LopkDocument3 pages2368 LopkigetisNo ratings yet
- DksoDocument2 pagesDksoigetisNo ratings yet
- TrainingPlan 003Document1 pageTrainingPlan 003igetisNo ratings yet
- Astral JournalDocument1 pageAstral JournalsimionNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 00000548c PDFDocument90 pages00000548c PDFlipNo ratings yet
- "1 Reva National Moot Court Championship": School of Legal StudiesDocument2 pages"1 Reva National Moot Court Championship": School of Legal StudiesIshan BramhbhattNo ratings yet
- Curriculum ProposalDocument38 pagesCurriculum ProposalMailyne Ventura Bacongco100% (3)
- Learn Verbs in EnglishDocument6 pagesLearn Verbs in EnglishCharmagne BorraNo ratings yet
- 11th Convocation List First ReleaseDocument44 pages11th Convocation List First Releasedip662004No ratings yet
- Acr Portfolio DayDocument4 pagesAcr Portfolio DayNica Salentes100% (2)
- Management Skills Training NeedsDocument5 pagesManagement Skills Training Needssahu050No ratings yet
- List of Members of The Browning Institute, Inc. Source: Browning Institute Studies, Vol. 12 (1984), Pp. 207-214 Published By: Cambridge University Press Accessed: 14-06-2020 09:58 UTCDocument9 pagesList of Members of The Browning Institute, Inc. Source: Browning Institute Studies, Vol. 12 (1984), Pp. 207-214 Published By: Cambridge University Press Accessed: 14-06-2020 09:58 UTCsamon sumulongNo ratings yet
- Eng 149 - Language Learning Materials Development HandoutDocument45 pagesEng 149 - Language Learning Materials Development HandoutHanifa PaloNo ratings yet
- Skilled Migration Assessment PolicyDocument16 pagesSkilled Migration Assessment PolicyHaneef MohamedNo ratings yet
- Fce Sample Papers 2008 WWW - Learninginstitute.chDocument117 pagesFce Sample Papers 2008 WWW - Learninginstitute.chpochaco4No ratings yet
- 4 Rizal's Childhood & 1st TripDocument46 pages4 Rizal's Childhood & 1st TripRain Storm PolgaderaNo ratings yet
- Indian Rupee SymbolDocument9 pagesIndian Rupee SymboljaihanumaninfotechNo ratings yet
- Earthquake Proof Structure ActivityDocument2 pagesEarthquake Proof Structure ActivityAJ CarranzaNo ratings yet
- LYNDSEY KUSTER - L-Blend-Foundational-FluencyDocument8 pagesLYNDSEY KUSTER - L-Blend-Foundational-FluencySharanya50% (2)
- Nature of Performance-Based AssessmentDocument3 pagesNature of Performance-Based AssessmentDarel GarzNo ratings yet
- Muhammad AURANGZEB: Academic QualificationDocument3 pagesMuhammad AURANGZEB: Academic QualificationyawiNo ratings yet
- Educational Psychology, Theories of PersonalitiesDocument32 pagesEducational Psychology, Theories of PersonalitiesNouman Hafeez100% (1)
- DLL CNFDocument2 pagesDLL CNFMARIA VICTORIA VELASCONo ratings yet
- Negovan CV Europass 20161202 Negovan enDocument1 pageNegovan CV Europass 20161202 Negovan enMihai NegovanNo ratings yet
- NORMAL DISTRIBUTION (Word Problem)Document9 pagesNORMAL DISTRIBUTION (Word Problem)Carl Jeremie LingatNo ratings yet
- Physical Fitness and Wellness 1Document3 pagesPhysical Fitness and Wellness 1Mac Postrano100% (1)
- Marcos Village Elementary School FunctionsDocument1 pageMarcos Village Elementary School FunctionsLeslie Joy Estardo Andrade100% (1)
- Developing Learner Autonomy in Vocabulary Learning For First-Year Mainstream Students at ED, ULIS, VNU. Tran Thi Huong Giang. QH.1.EDocument110 pagesDeveloping Learner Autonomy in Vocabulary Learning For First-Year Mainstream Students at ED, ULIS, VNU. Tran Thi Huong Giang. QH.1.EKavic100% (2)
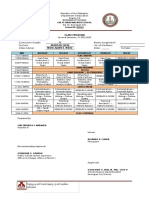
- Class Program (SY 2022-2023)Document12 pagesClass Program (SY 2022-2023)Cris Fredrich AndalizaNo ratings yet
- Freedom WritersDocument8 pagesFreedom WritersRacquel JohnsonNo ratings yet
- Clinical Reasoning Strategies in PTDocument19 pagesClinical Reasoning Strategies in PTamitesh_mpthNo ratings yet
- Seamo X Paper ADocument18 pagesSeamo X Paper Ad'Risdi ChannelNo ratings yet
- Readings in Philippine History: Analyzing Primary SourcesDocument22 pagesReadings in Philippine History: Analyzing Primary SourcesOmosay Gap ElgyzonNo ratings yet
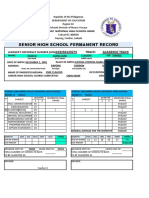
- Form 137 Senior HighDocument5 pagesForm 137 Senior HighZahjid Callang100% (1)