You might also like
- New Text DocumentDocument1 pageNew Text DocumentPande Indra PremanaNo ratings yet
- Study Report DHF and Dengue Fever, Untuk MuatDocument13 pagesStudy Report DHF and Dengue Fever, Untuk MuatPande Indra PremanaNo ratings yet
- Diagnosis Dan Tatalaksana: Nyoman PurwadiDocument26 pagesDiagnosis Dan Tatalaksana: Nyoman PurwadiPande Indra PremanaNo ratings yet
- 8 Rinitis Alergi Eng VersionDocument24 pages8 Rinitis Alergi Eng VersionPande Indra PremanaNo ratings yet
- Enzyme: Prof Bagiada CBM TeamDocument30 pagesEnzyme: Prof Bagiada CBM TeamPande Indra PremanaNo ratings yet
- Alimentary Disorders: Symptoms, Tests, and DiagnosesDocument1 pageAlimentary Disorders: Symptoms, Tests, and DiagnosesPande Indra PremanaNo ratings yet
- Learning Task Alimentary: Self AssessmentDocument1 pageLearning Task Alimentary: Self AssessmentPande Indra PremanaNo ratings yet
- Diagnosis and Management of AmebiasisDocument9 pagesDiagnosis and Management of AmebiasisPande Indra PremanaNo ratings yet
- Upper Alimentary Histology-2012Document23 pagesUpper Alimentary Histology-2012Pande Indra PremanaNo ratings yet
- Upper Alimentary Histology-2012Document23 pagesUpper Alimentary Histology-2012Pande Indra PremanaNo ratings yet
- Toxoplasmosis in PregnancyDocument13 pagesToxoplasmosis in PregnancyPande Indra PremanaNo ratings yet
- 6 ImunoTechniques 2012Document32 pages6 ImunoTechniques 2012Pande Indra PremanaNo ratings yet
- 17 Adrenal GlandDocument33 pages17 Adrenal GlandPande Indra PremanaNo ratings yet
- AA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarDocument26 pagesAA Gde Oka Sub-Lab/SMF Urologi FK - UNUD/RSUP Sanglah DenpasarPande Indra PremanaNo ratings yet
- 2 Organel LinaDocument34 pages2 Organel LinaMade WidianantaraNo ratings yet
- Doraemon Cartoon Summary: Nobita's Cat Robot Friend From The FutureDocument3 pagesDoraemon Cartoon Summary: Nobita's Cat Robot Friend From The FuturePande Indra PremanaNo ratings yet
- General Principles Physical Exam GuideDocument43 pagesGeneral Principles Physical Exam GuidePande Indra PremanaNo ratings yet
- Uroflowmetry ProcedureDocument1 pageUroflowmetry ProcedurePande Indra PremanaNo ratings yet
- Pathogenesis of Bacterial Infection Sem 3Document46 pagesPathogenesis of Bacterial Infection Sem 3Sheryl ElitaNo ratings yet
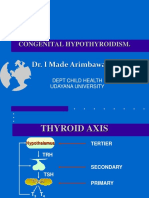
- 19 Congenital HipotiroidDocument21 pages19 Congenital HipotiroidPande Indra PremanaNo ratings yet
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocument38 pagesMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNo ratings yet
- 9 The Balinese TradmedCAMDocument43 pages9 The Balinese TradmedCAMPande Indra PremanaNo ratings yet
- 2 Total Ergonomic ApproachDocument25 pages2 Total Ergonomic ApproachPande Indra PremanaNo ratings yet
- Measurements of Morbidity and Mortality in A Population & Source of ErrorDocument38 pagesMeasurements of Morbidity and Mortality in A Population & Source of ErrorPande Indra PremanaNo ratings yet
- Describe of Definition of PolypharmacyDocument1 pageDescribe of Definition of PolypharmacyPande Indra PremanaNo ratings yet
- 19 Congenital HipotiroidDocument21 pages19 Congenital HipotiroidPande Indra PremanaNo ratings yet
- Treatment of Viral InfectionDocument33 pagesTreatment of Viral InfectionPande Indra PremanaNo ratings yet
- Rheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderDocument53 pagesRheumatoid Arthrirtis & Systemic Lupus Erythematosus: Interactive Lecture of Clinical Immune DisorderPande Indra PremanaNo ratings yet
- Achondroplasia Emedicine DKKDocument29 pagesAchondroplasia Emedicine DKKPande Indra PremanaNo ratings yet
- Genetic Counseling and Prenatal DiagnosisDocument13 pagesGenetic Counseling and Prenatal DiagnosisPande Indra Premana100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- I Am Sharing 'Pregnancy Shady' With YouDocument48 pagesI Am Sharing 'Pregnancy Shady' With YouNouran AlaaNo ratings yet
- Hong Kong A-Level Chemistry Book 3ADocument69 pagesHong Kong A-Level Chemistry Book 3AMARENG BERNABENo ratings yet
- Frozen DessertDocument3 pagesFrozen DessertcsqueilNo ratings yet
- FAI - Assignment Sheet (Both Assignments)Document5 pagesFAI - Assignment Sheet (Both Assignments)Wilson WongNo ratings yet
- Rumi and ReligionDocument2 pagesRumi and ReligionJustin LiewNo ratings yet
- RISO MZ Servicemanual EnglDocument438 pagesRISO MZ Servicemanual Englkuvalda2000_8645336367% (3)
- JKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Document3 pagesJKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Leong KmNo ratings yet
- Optitex Com Products 2d and 3d Cad SoftwareDocument12 pagesOptitex Com Products 2d and 3d Cad SoftwareFaathir Reza AvicenaNo ratings yet
- Philosophy of Disciple Making PaperDocument5 pagesPhilosophy of Disciple Making Paperapi-665038631No ratings yet
- Picco Tac 1095 N Hydrocarbon ResinDocument2 pagesPicco Tac 1095 N Hydrocarbon ResindevanandamqaNo ratings yet
- Haier's Performance Management in Other CulturesDocument8 pagesHaier's Performance Management in Other CulturesSubhransu SahooNo ratings yet
- Intro - S4HANA - Using - Global - Bike - Slides - MM - en - v3.3 MODDocument45 pagesIntro - S4HANA - Using - Global - Bike - Slides - MM - en - v3.3 MODMrThedjalexNo ratings yet
- PLC of MaggiDocument19 pagesPLC of Maggikrati agarwalNo ratings yet
- Literature Review Marketing StrategyDocument4 pagesLiterature Review Marketing Strategyc5td1cmc100% (1)
- Cls A310 Operations ManualDocument23 pagesCls A310 Operations ManualAntonio Ahijado Mendieta100% (2)
- Community Development A Critical Approach PDFDocument2 pagesCommunity Development A Critical Approach PDFNatasha50% (2)
- PoiconverterDocument2 pagesPoiconvertertaco6541No ratings yet
- User Manual - Numrolgy SoftwareDocument14 pagesUser Manual - Numrolgy SoftwareComputershastriNoproblem0% (1)
- Digital Burner Controller: Tbc2800 SeriesDocument4 pagesDigital Burner Controller: Tbc2800 SeriesSUDIP MONDALNo ratings yet
- Pressing and Finishing (Latest)Document8 pagesPressing and Finishing (Latest)Imran TexNo ratings yet
- Komposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefDocument11 pagesKomposit UHMWPE Sebagai Alternatif Bantalan Rel Kereta Api: Abel Evan, Alia Kristika, Farid Mulia LatiefAlia KristikaNo ratings yet
- MATH6113 - PPT5 - W5 - R0 - Applications of IntegralsDocument58 pagesMATH6113 - PPT5 - W5 - R0 - Applications of IntegralsYudho KusumoNo ratings yet
- English ProjectDocument10 pagesEnglish ProjectHarshman Singh HarshmanNo ratings yet
- 4WE10 New Series Directional Valves NG10Document9 pages4WE10 New Series Directional Valves NG10Paulo ArrudaNo ratings yet
- Anti-Anginal DrugsDocument39 pagesAnti-Anginal Drugspoonam rana100% (1)
- Polymer Science: Thermal Transitions in PolymersDocument20 pagesPolymer Science: Thermal Transitions in Polymerstanveer054No ratings yet
- EPM Mid Lecture 03 Chapt 1Document17 pagesEPM Mid Lecture 03 Chapt 1Partho Protim MondolNo ratings yet
- 4900 DatasheetDocument2 pages4900 DatasheetMakam Raghu100% (1)
- Applied Physics Mini Launcher Lab ReportDocument12 pagesApplied Physics Mini Launcher Lab ReportTalharashid RamzanNo ratings yet
- Financial Reporting Statement Analysis Project Report: Name of The Company: Tata SteelDocument35 pagesFinancial Reporting Statement Analysis Project Report: Name of The Company: Tata SteelRagava KarthiNo ratings yet