You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 1 Forthyron Pi 200 400 en PDFDocument1 page1 Forthyron Pi 200 400 en PDFjohnybarNo ratings yet
- NCPDocument14 pagesNCPclaidelynNo ratings yet
- Lab Exercise 5Document3 pagesLab Exercise 5Yeong-Ja KwonNo ratings yet
- Subjective: Diarrhea Related To Watery Short Term: IndependentDocument4 pagesSubjective: Diarrhea Related To Watery Short Term: IndependentEmma Lyn SantosNo ratings yet
- Geria NCPDocument4 pagesGeria NCPBrylle CapiliNo ratings yet
- Menstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleDocument6 pagesMenstrual Blood Derived Stem Cells and Their Scope in Regenerative Medicine A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- What Is Malnutrition?: WastingDocument6 pagesWhat Is Malnutrition?: WastingĐoan VõNo ratings yet
- Mapeh: Music - Arts - Physical Education - HealthDocument23 pagesMapeh: Music - Arts - Physical Education - HealthExtremelydarkness100% (1)
- Malawi Clinical HIV Guidelines 2019 Addendumversion 8.1Document28 pagesMalawi Clinical HIV Guidelines 2019 Addendumversion 8.1INNOCENT KHULIWANo ratings yet
- ZFN, TALEN, and CRISPR-Cas-based Methods For Genome EngineeringDocument9 pagesZFN, TALEN, and CRISPR-Cas-based Methods For Genome EngineeringRomina Tamara Gil RamirezNo ratings yet
- Kelseys ResumeDocument1 pageKelseys Resumeapi-401573835No ratings yet
- 2018 Surgical Rescue in Medical PatientsDocument11 pages2018 Surgical Rescue in Medical PatientsgiseladlrNo ratings yet
- National Geographic USA - January 2016Document148 pagesNational Geographic USA - January 2016stamenkovskib100% (4)
- The Nadi Vigyan by DR - Sharda Mishra MD (Proff. in Jabalpur Ayurved College)Document5 pagesThe Nadi Vigyan by DR - Sharda Mishra MD (Proff. in Jabalpur Ayurved College)Vivek PandeyNo ratings yet
- Lesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeDocument38 pagesLesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeSam GarciaNo ratings yet
- Liver Meeting Brochure 2016 PDFDocument4 pagesLiver Meeting Brochure 2016 PDFManas GhoshNo ratings yet
- Nursing Care of The Client With High-Risk Labor & DeliveryDocument10 pagesNursing Care of The Client With High-Risk Labor & DeliveryWilbert CabanbanNo ratings yet
- SNB Exam Sample Question Paper 2Document19 pagesSNB Exam Sample Question Paper 2Ketheesaran LingamNo ratings yet
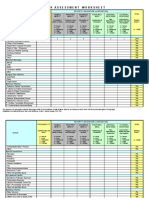
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Document4 pagesIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniNo ratings yet
- Orthobullets Foot and AnkleDocument88 pagesOrthobullets Foot and AnkleStevent Richardo100% (1)
- Sample Chapter of Assessment Made Incredibly Easy! 1st UK EditionDocument28 pagesSample Chapter of Assessment Made Incredibly Easy! 1st UK EditionLippincott Williams and Wilkins- Europe100% (1)
- Angina PectorisDocument17 pagesAngina PectorisRakesh Reddy100% (1)
- Gut Health Guidebook 9 22Document313 pagesGut Health Guidebook 9 2219760227No ratings yet
- Pathophysiology of Ischemic Stroke FinalDocument3 pagesPathophysiology of Ischemic Stroke FinalAcohCChao67% (3)
- Anatomi & Fisiologi Sistem RespirasiDocument57 pagesAnatomi & Fisiologi Sistem RespirasijuliandiNo ratings yet
- Páginas de Rockwood Fraturas em Adultos, 8ed3Document51 pagesPáginas de Rockwood Fraturas em Adultos, 8ed3Estevão CananNo ratings yet
- Fertilization Reflection PaperDocument2 pagesFertilization Reflection PaperCrisandro Allen Lazo100% (2)
- PowersDocument14 pagesPowersIvan SokolovNo ratings yet
- Resveratrol and Its Effects On Human Health and LongevityDocument367 pagesResveratrol and Its Effects On Human Health and LongevityArnulfo Yu LanibaNo ratings yet
- Complications and Failures of ImplantsDocument35 pagesComplications and Failures of ImplantssavNo ratings yet