You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Clinical CaseDocument10 pagesClinical CaseRoberto RamosNo ratings yet
- Soap RoutineDocument3 pagesSoap RoutineRoberto Ramos100% (1)
- Case 3Document8 pagesCase 3Roberto RamosNo ratings yet
- Case 2 AlmostDocument8 pagesCase 2 AlmostRoberto RamosNo ratings yet
- Rhie Full OcrDocument120 pagesRhie Full OcrRoberto RamosNo ratings yet
- Universidad de Puerto Rico Mail - (No Subject)Document77 pagesUniversidad de Puerto Rico Mail - (No Subject)Roberto RamosNo ratings yet
- History: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasDocument9 pagesHistory: Chief Complaint: History of Present Illness: Patient Is A 59 Year Old G6 P1051 Woman Who Is An Inmate That WasRoberto RamosNo ratings yet
- McCowan SGA RiskFactors BJOG 2010Document9 pagesMcCowan SGA RiskFactors BJOG 2010Roberto RamosNo ratings yet
- Long Case Presentation FINAL-33Document7 pagesLong Case Presentation FINAL-33Roberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Paciente 3Document80 pagesPaciente 3Roberto RamosNo ratings yet
- Long Case Presentation FINAL-5Document7 pagesLong Case Presentation FINAL-5Roberto RamosNo ratings yet
- Radio ObGynDocument1 pageRadio ObGynRoberto RamosNo ratings yet
- Repaso ShelfDocument135 pagesRepaso ShelfRoberto RamosNo ratings yet
- Progress Note Osce - HIV (1) - 2Document1 pageProgress Note Osce - HIV (1) - 2Roberto RamosNo ratings yet
- SEPSIS Case 2014 - August-2Document45 pagesSEPSIS Case 2014 - August-2Roberto RamosNo ratings yet
- Final - Answers of Ekg QuizDocument46 pagesFinal - Answers of Ekg QuizRoberto RamosNo ratings yet
- "Repaso" Shelf OB - GYN 2 2Document9 pages"Repaso" Shelf OB - GYN 2 2Roberto RamosNo ratings yet
- Untitled Spreadsheet 2Document4 pagesUntitled Spreadsheet 2Roberto RamosNo ratings yet
- Universidad Puerto Rico Manual 1415Document161 pagesUniversidad Puerto Rico Manual 1415Roberto RamosNo ratings yet
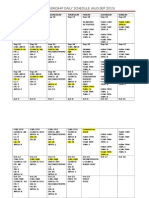
- Ob-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Document3 pagesOb-Gyn Clerkship Daily Schedule (Aug-Sep 2015)Roberto RamosNo ratings yet
- Health Maintenance Cases For Discussion-5Document4 pagesHealth Maintenance Cases For Discussion-5Roberto RamosNo ratings yet
- DR - Umpierrere2012 2013 4Document70 pagesDR - Umpierrere2012 2013 4Roberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- There Is Been An Overlooked But Important TopicDocument2 pagesThere Is Been An Overlooked But Important TopicRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- HTTPDocument1 pageHTTPRoberto RamosNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Omnibus Motion (Motion To Re-Open, Admit Answer and Delist: Republic of The PhilippinesDocument6 pagesOmnibus Motion (Motion To Re-Open, Admit Answer and Delist: Republic of The PhilippinesHIBA INTL. INC.No ratings yet
- Business Research Chapter 1Document27 pagesBusiness Research Chapter 1Toto H. Ali100% (2)
- Vol. III (B) - FANSDocument8 pagesVol. III (B) - FANSKhaled ELSaftawyNo ratings yet
- World Price List 2014: Adventys Induction Counter TopsDocument4 pagesWorld Price List 2014: Adventys Induction Counter TopsdiogocorollaNo ratings yet
- Dampak HidrokarbonDocument10 pagesDampak HidrokarbonfikririansyahNo ratings yet
- Robber Bridegroom Script 1 PDFDocument110 pagesRobber Bridegroom Script 1 PDFRicardo GarciaNo ratings yet
- 4aeaconditionals 110228122737 Phpapp01Document24 pages4aeaconditionals 110228122737 Phpapp01Luis Fernando Ponce JimenezNo ratings yet
- Articles of Incorporation 2Document5 pagesArticles of Incorporation 2Marcos DmitriNo ratings yet
- Business Emails - Style and StructureDocument4 pagesBusiness Emails - Style and StructureFall Eljed100% (1)
- Gothic Fiction Oliver TwistDocument3 pagesGothic Fiction Oliver TwistTaibur RahamanNo ratings yet
- Chapter 4 Lesson ProperDocument44 pagesChapter 4 Lesson ProperWenceslao LynNo ratings yet
- Computer Awareness: Special Edition E-BookDocument54 pagesComputer Awareness: Special Edition E-BookTanujit SahaNo ratings yet
- Jingle KKKKDocument80 pagesJingle KKKKCristina Joy Valdez AndresNo ratings yet
- Net 2020Document48 pagesNet 2020Krishan pandeyNo ratings yet
- On Evil - Terry EagletonDocument44 pagesOn Evil - Terry EagletonconelcaballocansadoNo ratings yet
- SPECIAL POWER OF ATTORNEY To JeffDocument2 pagesSPECIAL POWER OF ATTORNEY To JeffTom SumawayNo ratings yet
- Multigrade Lesson Plan MathDocument7 pagesMultigrade Lesson Plan MathArmie Yanga HernandezNo ratings yet
- Chelsea Bellomy ResumeDocument1 pageChelsea Bellomy Resumeapi-301977181No ratings yet
- Case Study - Lucky Cement and OthersDocument16 pagesCase Study - Lucky Cement and OthersKabeer QureshiNo ratings yet
- Chapter 11 Towards Partition Add Pakistan 1940-47Document5 pagesChapter 11 Towards Partition Add Pakistan 1940-47LEGEND REHMAN OPNo ratings yet
- Recollections From Pine Gulch QuestionsDocument2 pagesRecollections From Pine Gulch Questionsoliver abramsNo ratings yet
- MANITOUDocument2 pagesMANITOUmozollis22No ratings yet
- Pam ApplicationDocument3 pagesPam Applicationapi-534834656No ratings yet
- 4TES-9Y 20KW With InverterDocument4 pages4TES-9Y 20KW With InverterPreeti gulatiNo ratings yet
- Data Types of SQL (Oracle) : Provided By: - Pronab Kumar AdhikariDocument1 pageData Types of SQL (Oracle) : Provided By: - Pronab Kumar AdhikariMannan AhmadNo ratings yet
- Computer Science Past Papers MCQS SolvedDocument24 pagesComputer Science Past Papers MCQS SolvedLEGAL AFFAIRS DIVISION100% (1)
- Holistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaDocument4 pagesHolistic Centre: Case Study 1 - Osho International Meditation Centre, Pune, IndiaPriyesh Dubey100% (2)
- Banking - BPI V Sps Yu 2010Document8 pagesBanking - BPI V Sps Yu 2010roy dNo ratings yet
- War: Causation of War, Total War, Limited War, Strategic Culture: Determinants of Strategic Culture Deterrence: Theory and Practice With SpecialDocument52 pagesWar: Causation of War, Total War, Limited War, Strategic Culture: Determinants of Strategic Culture Deterrence: Theory and Practice With SpecialMazhar HussainNo ratings yet
- A Letter From Sir William R. Hamilton To John T. Graves, EsqDocument7 pagesA Letter From Sir William R. Hamilton To John T. Graves, EsqJoshuaHaimMamouNo ratings yet