You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Active RecreationDocument5 pagesActive RecreationVhannie AcquiatanNo ratings yet
- EN Sample Paper 17 Unsolved MysteryDocument10 pagesEN Sample Paper 17 Unsolved MysteryShankhadeep ChoudhuryNo ratings yet
- Iron AllowancesDocument6 pagesIron AllowancesJenie Munar RosarioNo ratings yet
- 12 Physical Education Chapter 3Document24 pages12 Physical Education Chapter 3akanksha nayanNo ratings yet
- PWC Social Determinants of HealthDocument36 pagesPWC Social Determinants of HealthAnam FatimaNo ratings yet
- The Gabriel Method: The Revolutionary Diet-Free Way To Totally Transform Your Body - Jon GabrielDocument5 pagesThe Gabriel Method: The Revolutionary Diet-Free Way To Totally Transform Your Body - Jon Gabrielhukomeso0% (2)
- Microsoft Word - Stewart FAC 6-12-16 - WebsiteDocument32 pagesMicrosoft Word - Stewart FAC 6-12-16 - WebsiteEmanuele GiasiNo ratings yet
- Crisis ManagementDocument17 pagesCrisis ManagementAnonymous vNbLLN2iNo ratings yet
- Book StickerDocument4 pagesBook Stickerilanabiela90No ratings yet
- Philippine Festivals and Traditions MAPEH TestDocument19 pagesPhilippine Festivals and Traditions MAPEH TestGigi Reyes SisonNo ratings yet
- ESPGHAN Sugar Intake GuideDocument4 pagesESPGHAN Sugar Intake Guidedayanita1221No ratings yet
- Assessment and Management of Patients With ObesityDocument2 pagesAssessment and Management of Patients With ObesityaliNo ratings yet
- Performance of broiler chickens fed on Moringa oleifera leaf meal supplemented dietsDocument8 pagesPerformance of broiler chickens fed on Moringa oleifera leaf meal supplemented dietsMariz BallonNo ratings yet
- New Sip TemplateDocument84 pagesNew Sip TemplateOscar MatelaNo ratings yet
- Exercise Habit Among StudentsDocument30 pagesExercise Habit Among StudentsDaniel Hoe Wen ChuanNo ratings yet
- Healthy Lifestyle Changes to Combat ObesityDocument3 pagesHealthy Lifestyle Changes to Combat ObesityNorsyakira NawirNo ratings yet
- EBM Review Units1 4Document8 pagesEBM Review Units1 4Aissha ArifNo ratings yet
- Essential guide to anthropometry for child nutritionDocument2 pagesEssential guide to anthropometry for child nutritionChristian DaivaNo ratings yet
- Connected: The Six Rules of Social Networks and How They Shape Our LivesDocument5 pagesConnected: The Six Rules of Social Networks and How They Shape Our LivesJed Diamond100% (3)
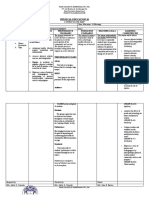
- Curri Map Pe 10Document9 pagesCurri Map Pe 10Arnel BoholstNo ratings yet
- Eat Right... Transform Your Body-1Document34 pagesEat Right... Transform Your Body-1ozokwelu ebere100% (1)
- Research ProposalDocument36 pagesResearch ProposalShakilaNo ratings yet
- John W. Santrock - Life-Span Development-McGraw-Hill Education (2018) - 399-461-DikonversiDocument23 pagesJohn W. Santrock - Life-Span Development-McGraw-Hill Education (2018) - 399-461-DikonversiElsfrdlNo ratings yet
- 02 Nutrition and Nutritional DisordersDocument114 pages02 Nutrition and Nutritional DisordersMateen ShukriNo ratings yet
- Importance of PE for Weight Control, Stress Relief, Self-ConfidenceDocument6 pagesImportance of PE for Weight Control, Stress Relief, Self-ConfidenceJoe D'AmbrosioNo ratings yet
- BCP Evaluation FormDocument1 pageBCP Evaluation Formblackspyder1081No ratings yet
- National Food Strategy Recommendations in FullDocument73 pagesNational Food Strategy Recommendations in FullNeil ShellardNo ratings yet
- 10 Final Mapeh P.E. 10 Q2 M1 Week 5Document16 pages10 Final Mapeh P.E. 10 Q2 M1 Week 5Pedro GojoNo ratings yet
- Meigas: Nickname: Guajonas, Bruxas and Especially Xuxonas, Referring To His DarkDocument4 pagesMeigas: Nickname: Guajonas, Bruxas and Especially Xuxonas, Referring To His DarkJack RubyNo ratings yet
- Nutr 425 Diabetes AdimeDocument3 pagesNutr 425 Diabetes Adimeapi-341618058No ratings yet