You might also like
- Sexually Transmitted Infections-5Document5 pagesSexually Transmitted Infections-5diko_nalNo ratings yet
- Lymphogranuloma Venereum (LGV) - Background, Pathophysiology, EpidemiologyDocument7 pagesLymphogranuloma Venereum (LGV) - Background, Pathophysiology, EpidemiologyARHNo ratings yet
- Rabies FinalDocument18 pagesRabies FinalPrem SinghNo ratings yet
- Viral and Protozoal Infection in PregnancyDocument58 pagesViral and Protozoal Infection in Pregnancyjyoti kunduNo ratings yet
- Window Period: Terms Related To Hiv /aidsDocument10 pagesWindow Period: Terms Related To Hiv /aidsKavi rajputNo ratings yet
- Diaz & Estrael Sc23 VirologyDocument69 pagesDiaz & Estrael Sc23 VirologyJohn Rafael DiazNo ratings yet
- 24.11.09 PPT On Intrauterine InfectionDocument57 pages24.11.09 PPT On Intrauterine InfectionDhara Meena90% (10)
- Viral Hepatitis: Dr. Staar Mohammed QaderDocument60 pagesViral Hepatitis: Dr. Staar Mohammed QaderMohammed R.HusseinNo ratings yet
- Hepatitis - An Overview: Dr. JayalakshmiDocument77 pagesHepatitis - An Overview: Dr. JayalakshmiNithin SundarNo ratings yet
- Congenital Viral InfectionsDocument43 pagesCongenital Viral Infectionsannie1970100% (1)
- Exually Ransmitted IseasesDocument52 pagesExually Ransmitted Iseasesjanjan eresoNo ratings yet
- Virology: StructureDocument13 pagesVirology: StructureJoan BabieraNo ratings yet
- Sexually Transmitted Deisease: There Are Three Different Kinds of STDS: Bacterial, Viral, and ParasiticDocument22 pagesSexually Transmitted Deisease: There Are Three Different Kinds of STDS: Bacterial, Viral, and ParasiticClara Marie GonzaludoNo ratings yet
- Diagnosis of Viral Infection (2021-2022)Document21 pagesDiagnosis of Viral Infection (2021-2022)Fahim JaniNo ratings yet
- AIDS Teaching ModuleDocument122 pagesAIDS Teaching Moduletummalapalli venkateswara raoNo ratings yet
- Human Immunodeficiency Virus HIVDocument14 pagesHuman Immunodeficiency Virus HIVAdam ChungNo ratings yet
- Chancroid: Ducreyi Is Available in The United States, But SuchDocument8 pagesChancroid: Ducreyi Is Available in The United States, But Suchwicak_spNo ratings yet
- Infections in Pregnancy 2Document26 pagesInfections in Pregnancy 2Karanand Choppingboardd Rahgav MaharajNo ratings yet
- Part 2 of Medical VirologyDocument113 pagesPart 2 of Medical Virologygatete samNo ratings yet
- By: Evita Mayasari, DR., Mkes.: Microbiology Department Medical School University of Sumatera UtaraDocument65 pagesBy: Evita Mayasari, DR., Mkes.: Microbiology Department Medical School University of Sumatera UtaraDwi Meutia IndriatiNo ratings yet
- Lecture 2 - Diagnostic Tests in VirologyDocument26 pagesLecture 2 - Diagnostic Tests in VirologyJeanPaule JoumaaNo ratings yet
- Appropriate Clinical Specimens Collection and Transport For Diagnostic VirologyDocument48 pagesAppropriate Clinical Specimens Collection and Transport For Diagnostic Virologylong thomNo ratings yet
- Laboratory Diagnosis of Viral InfectionsDocument71 pagesLaboratory Diagnosis of Viral InfectionsMunazzaNo ratings yet
- Congenital SyphilisDocument22 pagesCongenital SyphilisJuliana MariaNo ratings yet
- Lab 1 Serology: Collection, Preparation, Processing and Transport of Serological SpecimensDocument18 pagesLab 1 Serology: Collection, Preparation, Processing and Transport of Serological SpecimensGhadi AbdalazizNo ratings yet
- Chlamydia PosterDocument1 pageChlamydia PosterCharlene WongNo ratings yet
- StdsDocument14 pagesStdsJumar Divinagracia DimpasNo ratings yet
- R - Bio-Rad Geenius HIV 1 2 Supplemental Test SSE FinalDocument29 pagesR - Bio-Rad Geenius HIV 1 2 Supplemental Test SSE FinalromerilloNo ratings yet
- 5 - Viral DiagnosisDocument24 pages5 - Viral DiagnosisAyeshaNo ratings yet
- Lecture 3 - HerpesvirusesDocument48 pagesLecture 3 - HerpesvirusesJeanPaule JoumaaNo ratings yet
- 04 - Typhoid FeverDocument35 pages04 - Typhoid Feversoheil100% (1)
- Infectious Disease in PregnancyDocument21 pagesInfectious Disease in PregnancyLauren McrobertsNo ratings yet
- Human Papilloma VirusDocument3 pagesHuman Papilloma Virusxwendnla russiaNo ratings yet
- HIV and AIDS - PDF 2Document26 pagesHIV and AIDS - PDF 2Cheska JunturaNo ratings yet
- Biology ProjectDocument18 pagesBiology Projecthahirwar35No ratings yet
- Lab 9. Sample CollectionDocument23 pagesLab 9. Sample CollectionSuzan AbdNo ratings yet
- 15medically Important Viruses PDFDocument75 pages15medically Important Viruses PDFdan ghaNo ratings yet
- 2.dynamic of Diseases Transmission - Copy 2Document54 pages2.dynamic of Diseases Transmission - Copy 2Fatimah Abd-alhadiNo ratings yet
- Mikrobiologi Virus ArthropodeDocument55 pagesMikrobiologi Virus Arthropodeakun scribNo ratings yet
- Management of HIV in Pregnant WomenDocument32 pagesManagement of HIV in Pregnant WomenKokoland KukusNo ratings yet
- Chapter 24 VirusesDocument3 pagesChapter 24 VirusesBlairNo ratings yet
- Celiac Disease in ChildrenDocument59 pagesCeliac Disease in Childrend-fbuser-57045067No ratings yet
- CytomegalovirusDocument2 pagesCytomegalovirusrae_ramirez25No ratings yet
- Virology Pre FinalDocument5 pagesVirology Pre FinalScarlet EmpressNo ratings yet
- Chapter II VirologyDocument116 pagesChapter II VirologyTofikNo ratings yet
- Sexually Transmitted DiseasesDocument19 pagesSexually Transmitted DiseasesJayvah EstrellaNo ratings yet
- Flotation LabDocument17 pagesFlotation LabChinyere ObiNo ratings yet
- Sexually Transmitted DiseaseDocument38 pagesSexually Transmitted Diseaserana arslanNo ratings yet
- Principles and Practice of AsepsisDocument24 pagesPrinciples and Practice of AsepsisMuhammad AdamNo ratings yet
- Haemophilus DucreyiDocument15 pagesHaemophilus DucreyichristieNo ratings yet
- Opportunistic Amoeba Facultative ParasitesDocument25 pagesOpportunistic Amoeba Facultative ParasitesLizeth Querubin100% (10)
- Nepal National Hiv Testing and Treatment Guidelines 2022Document158 pagesNepal National Hiv Testing and Treatment Guidelines 2022medical ChyNo ratings yet
- Breast Cancer Awareness: Dr. Amber RasheedDocument34 pagesBreast Cancer Awareness: Dr. Amber RasheedAmber Gulamani100% (1)
- Virology Respiratory VirusesDocument6 pagesVirology Respiratory VirusesHisham ChomanyNo ratings yet
- Hiv Infection and AidsDocument51 pagesHiv Infection and Aidspokhara gharipatanNo ratings yet
- Dynamics of Disease TransmissionDocument30 pagesDynamics of Disease TransmissionSyed Sanan shahNo ratings yet
- Immunoparasitology and Fungal ImmunityDocument31 pagesImmunoparasitology and Fungal ImmunityShakti PatelNo ratings yet
- Sexually Transmitted DiseasesDocument17 pagesSexually Transmitted DiseasesChrystele Ann Ramilo100% (1)
- Determining Gravidity and Parity: I. GravidaDocument6 pagesDetermining Gravidity and Parity: I. GravidaDanica CorpuzNo ratings yet
- Case Study BuenavistaDocument5 pagesCase Study BuenavistaGen-Gen Belenio BillonesNo ratings yet
- Training Manual Hypertensive Disorder in Pregnancy 3rd Edition 2018 PDFDocument140 pagesTraining Manual Hypertensive Disorder in Pregnancy 3rd Edition 2018 PDFJaspreet KaurNo ratings yet
- Thyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeDocument14 pagesThyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeNoraNo ratings yet
- Pregnancy in A Patient With Recurrent GlioblastomaDocument6 pagesPregnancy in A Patient With Recurrent GlioblastomaNoraNo ratings yet
- Antenatal Care and Its Effect On Risk of PihDocument11 pagesAntenatal Care and Its Effect On Risk of PihNoraNo ratings yet
- Anaemia On First Trimester PregnancyDocument11 pagesAnaemia On First Trimester PregnancyNoraNo ratings yet
- Stress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthDocument10 pagesStress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthNoraNo ratings yet
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDocument11 pagesAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNo ratings yet
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDocument11 pagesAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNo ratings yet
- Preterm DeliveryDocument12 pagesPreterm DeliveryNoraNo ratings yet
- Preterm DeliveryDocument12 pagesPreterm DeliveryNoraNo ratings yet
- Female Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)Document8 pagesFemale Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)NoraNo ratings yet
- Pra Penulisan Bi Karangan UpsrDocument111 pagesPra Penulisan Bi Karangan Upsropheliaviolet100% (1)
- Large For Gestational AgeDocument23 pagesLarge For Gestational AgeNoraNo ratings yet
- Large For Gestational AgeDocument23 pagesLarge For Gestational AgeNoraNo ratings yet
- Nursing ManagerDocument30 pagesNursing ManagerNoraNo ratings yet
- Active Management of Pregnant Cancer PatientDocument9 pagesActive Management of Pregnant Cancer PatientNoraNo ratings yet
- Female Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)Document8 pagesFemale Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)NoraNo ratings yet
- Orientation ListDocument1 pageOrientation ListNoraNo ratings yet
- Menu Makanan Untuk Pesakit Hospital: IsninDocument2 pagesMenu Makanan Untuk Pesakit Hospital: IsninNoraNo ratings yet
- Bakri Balloon PDFDocument5 pagesBakri Balloon PDFNoraNo ratings yet
- End of Life Care BrochureDocument2 pagesEnd of Life Care BrochureNoraNo ratings yet
- Factors Affecting Maternal Perception of Fetal MovementsDocument9 pagesFactors Affecting Maternal Perception of Fetal MovementsNoraNo ratings yet
- 4.2preparing For PregnancyDocument5 pages4.2preparing For PregnancyNoraNo ratings yet
- Injections SiteDocument10 pagesInjections SiteNora100% (2)
- 47.anemia 2012 EditionDocument480 pages47.anemia 2012 EditionRodica Badea100% (1)
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDocument93 pagesKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNo ratings yet
- Prenatal CareDocument129 pagesPrenatal CareNora100% (1)
- Preuritic Urticarial Papule and Plaque of Pregnancy PDFDocument5 pagesPreuritic Urticarial Papule and Plaque of Pregnancy PDFNoraNo ratings yet
- Detection Methods and Knowledge Levels Regarding Breast CancerDocument41 pagesDetection Methods and Knowledge Levels Regarding Breast CancerNora100% (1)
- Pressure Points - Postnatal Care Planning PDFDocument15 pagesPressure Points - Postnatal Care Planning PDFNoraNo ratings yet
- Seminar On Preventive ObstetricsDocument49 pagesSeminar On Preventive ObstetricsRini Robert100% (3)
- Oral SexDocument18 pagesOral SexVerlana Garcia100% (1)
- Syphilinum. (Luesinum.) - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANT PDFDocument24 pagesSyphilinum. (Luesinum.) - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANT PDFHarrison DavidsonNo ratings yet
- Kode Icd 10Document876 pagesKode Icd 10Angga WarismanNo ratings yet
- Im Boards Rationalized ExamDocument21 pagesIm Boards Rationalized Examesbat07No ratings yet
- Midterm Module SocSci 111Document40 pagesMidterm Module SocSci 111Frances Georgina FabaleNo ratings yet
- Obg MCQS PDFDocument11 pagesObg MCQS PDFPreeti ChouhanNo ratings yet
- Pityriasis RoseaDocument23 pagesPityriasis RoseaYellyasta Siusiu Imran100% (3)
- Primary SyphilisDocument3 pagesPrimary SyphilisEqah TajuddinNo ratings yet
- NSTPDocument2 pagesNSTPBernadette ArrojoNo ratings yet
- Country Progress Report On: Hiv/AidsDocument45 pagesCountry Progress Report On: Hiv/AidsDineish MurugaiahNo ratings yet
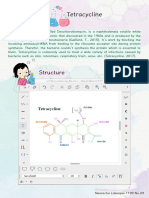
- TetracyclineDocument5 pagesTetracyclineapi-296073547No ratings yet
- Systemic Disease and Their Oral ManifestationsDocument80 pagesSystemic Disease and Their Oral ManifestationsRakshya ShresthaNo ratings yet
- Written Part AlfavitikaDocument24 pagesWritten Part AlfavitikaShanna MitchellNo ratings yet
- Penyakit Menular SeksualDocument83 pagesPenyakit Menular SeksualIvan Ho0% (1)
- Medical Ethics Accounts of Ground Breaking Cases 7Th Edition Pence Test Bank Full Chapter PDFDocument28 pagesMedical Ethics Accounts of Ground Breaking Cases 7Th Edition Pence Test Bank Full Chapter PDFStephanieMckayeqwr100% (11)
- MedSurg II Post TestDocument19 pagesMedSurg II Post TestMaria Luz S. RulonaNo ratings yet
- Question 1Document66 pagesQuestion 1DurgaMadhab TripathyNo ratings yet
- Nbme 100Document11 pagesNbme 100stndNo ratings yet
- SyphilisDocument32 pagesSyphilisSabrina Porquiado Magañan SNNo ratings yet
- TORCH in PregnancyDocument63 pagesTORCH in PregnancyKinjal VasavaNo ratings yet
- Is Lab P4 - Serologic Tests For SyphilisDocument4 pagesIs Lab P4 - Serologic Tests For SyphilisDanielle Anne LambanNo ratings yet
- Clinical Manifestations and Treatment of Syphilis - UpToDateDocument2 pagesClinical Manifestations and Treatment of Syphilis - UpToDateCarmenDuganNo ratings yet
- STDs in Sangamon CountyDocument15 pagesSTDs in Sangamon CountyNewsTeam20No ratings yet
- Acterial Iseases: Prepared By: Dr. Rea CorpuzDocument63 pagesActerial Iseases: Prepared By: Dr. Rea CorpuzMedecine Dentaire100% (2)
- Gibson Miller R - A Synopsis of Homoeopathic Philosophy 1900Document21 pagesGibson Miller R - A Synopsis of Homoeopathic Philosophy 1900Rajesh Rajendran100% (2)
- Manifestations of Miasms in DiseaseDocument3 pagesManifestations of Miasms in Diseaselydia2301100% (2)
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
- Antenatal CareDocument19 pagesAntenatal CareIshika RoyNo ratings yet
- TORCH in PregnancyDocument63 pagesTORCH in PregnancySaRah AmiThia SaRi BuLanNo ratings yet