You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PNLE Sample Test QuestionsDocument12 pagesPNLE Sample Test QuestionsHam-Ham LootNo ratings yet
- Journ 3Document9 pagesJourn 3ハルァン ファ烏山No ratings yet
- OCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004BradfordDocument244 pagesOCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004Bradfordハルァン ファ烏山No ratings yet
- OCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004BradfordDocument244 pagesOCR BasicOphthalmology4MedicalStudents&PrimaryCareResidents8ed2004Bradfordハルァン ファ烏山No ratings yet
- Journ 4Document29 pagesJourn 4ハルァン ファ烏山No ratings yet
- Preho 1Document1 pagePreho 1ハルァン ファ烏山No ratings yet
- OCR KaplanUSMLEStep2 Gastroenterology2001Document37 pagesOCR KaplanUSMLEStep2 Gastroenterology2001ハルァン ファ烏山No ratings yet
- FilesDocument21 pagesFilesハルァン ファ烏山No ratings yet
- WidgetDocument9 pagesWidgetRavikiran V SurpurNo ratings yet
- Eula ENUDocument2 pagesEula ENUMaylyn Valencia A.No ratings yet
- ReadmeDocument30 pagesReadmeoyanbleNo ratings yet
- WidgetDocument9 pagesWidgetRavikiran V SurpurNo ratings yet
- ReadmeDocument304 pagesReadmeハルァン ファ烏山No ratings yet
- Eula ENUDocument2 pagesEula ENUMaylyn Valencia A.No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 5Document1 pageMoriya Shrine - Akyu's Untouched Score Vol. 5ハルァン ファ烏山No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 3Document1 pageMoriya Shrine - Akyu's Untouched Score Vol. 3ハルァン ファ烏山No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 4Document1 pageMoriya Shrine - Akyu's Untouched Score Vol. 4ハルァン ファ烏山No ratings yet
- Preeclampsia - Syndrome or DiseaseDocument8 pagesPreeclampsia - Syndrome or Diseaseハルァン ファ烏山No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 1 Disc ADocument1 pageMoriya Shrine - Akyu's Untouched Score Vol. 1 Disc Aハルァン ファ烏山No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 2Document1 pageMoriya Shrine - Akyu's Untouched Score Vol. 2ハルァン ファ烏山No ratings yet
- Moriya Shrine - Akyu's Untouched Score Vol. 1 Disc BDocument1 pageMoriya Shrine - Akyu's Untouched Score Vol. 1 Disc Bハルァン ファ烏山No ratings yet
- Premature Rupture of Membrane at Term - Early Induction Versus Expectant ManagementDocument4 pagesPremature Rupture of Membrane at Term - Early Induction Versus Expectant Managementハルァン ファ烏山No ratings yet
- Obstetric Outcomes of Mothers Previously Exposed To Sexual ViolenceDocument12 pagesObstetric Outcomes of Mothers Previously Exposed To Sexual Violenceハルァン ファ烏山No ratings yet
- Neonatal Outcome in Preterm Deliveries Between 23 and 27 Weeks' Gestation With and Without Preterm Premature Rupture of Membranes PDFDocument5 pagesNeonatal Outcome in Preterm Deliveries Between 23 and 27 Weeks' Gestation With and Without Preterm Premature Rupture of Membranes PDFハルァン ファ烏山No ratings yet
- GA by Ultrasound SOGCDocument11 pagesGA by Ultrasound SOGCBrendaNo ratings yet
- AssetDocument31 pagesAssetハルァン ファ烏山No ratings yet
- AssetDocument11 pagesAssetハルァン ファ烏山No ratings yet
- AssetDocument10 pagesAssetハルァン ファ烏山No ratings yet
- Nej Mo A 1508606Document15 pagesNej Mo A 1508606ハルァン ファ烏山No ratings yet
- Councelling and History TakingDocument5 pagesCouncelling and History TakingbashingarNo ratings yet
- IcdDocument21 pagesIcdVicky AprizanoNo ratings yet
- Fetal Monitoring Technology: Application NoteDocument8 pagesFetal Monitoring Technology: Application NoteCarlos MedikalNo ratings yet
- Midwifery InfographicDocument1 pageMidwifery InfographicAnie NurrahmianiNo ratings yet
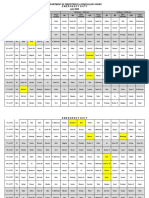
- Department of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020Document3 pagesDepartment of Obstetrics & Gynecology-Wwrc Emergency Duty July 2020noorNo ratings yet
- High Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyDocument79 pagesHigh Risk Pregnancy:: A Woman Who Develops A Complication of PregnancyMike Faustino SolangonNo ratings yet
- Acog Parto Vaginal QX PDFDocument11 pagesAcog Parto Vaginal QX PDFAnghelino Jesus Meza CentenoNo ratings yet
- Assisted DeliveryDocument20 pagesAssisted DeliverySaid Said (ابو خالد)No ratings yet
- Abdominal Palpation & Examination in Pregnancy 5.0 PDFDocument11 pagesAbdominal Palpation & Examination in Pregnancy 5.0 PDFPalaniswami Palaniswami100% (1)
- S2 2016 354314 BibliographyDocument3 pagesS2 2016 354314 BibliographyFezra JoesfaNo ratings yet
- Knowledge, Attitude, and Practice of Pregnant Mothers Regarding Exercise During Pregnancy in Mothers Who Have ANC Follow-Up, Addis Ababa, EthiopiaDocument24 pagesKnowledge, Attitude, and Practice of Pregnant Mothers Regarding Exercise During Pregnancy in Mothers Who Have ANC Follow-Up, Addis Ababa, EthiopiaBEREKETNo ratings yet
- Facts About AbortionDocument5 pagesFacts About Abortiontristan avyNo ratings yet
- Anatomical Causes of Bad Obstetric HistoryDocument3 pagesAnatomical Causes of Bad Obstetric Historykyle31No ratings yet
- Resume Obs 21-27 Februari 21Document6 pagesResume Obs 21-27 Februari 21imamsantos1191No ratings yet
- WW.05.21 Forceps Assisted Vaginal DeliveryDocument3 pagesWW.05.21 Forceps Assisted Vaginal DeliveryLani Munawir Holis HolisNo ratings yet
- The Bishop ScoreDocument3 pagesThe Bishop ScoreJheanAlphonsineT.MeansNo ratings yet
- Vacuum-Assisted Vaginal Delivery: Echnique EviewDocument13 pagesVacuum-Assisted Vaginal Delivery: Echnique Eviewgingerblue08No ratings yet
- Antepartum HaemorrhageDocument45 pagesAntepartum HaemorrhageGeorge C. KasondaNo ratings yet
- LATIHAN 15.3 - Perkembangan Fetus Manusia: Trialkelantan2019Document2 pagesLATIHAN 15.3 - Perkembangan Fetus Manusia: Trialkelantan2019myra zainalNo ratings yet
- Population Development Division Brho Monitoring and AccomplishmentDocument3 pagesPopulation Development Division Brho Monitoring and AccomplishmentBarangay UbaliwNo ratings yet
- Who FRH MSM 96.24Document58 pagesWho FRH MSM 96.24crushnaNo ratings yet
- Umbilical Cord ProlapseDocument5 pagesUmbilical Cord Prolapseangga hergaNo ratings yet
- 1 s2.0 S0266613816301152 MainDocument8 pages1 s2.0 S0266613816301152 MainsyamsuryadiNo ratings yet
- 10 Steps To Successful Breastfeeding 2Document39 pages10 Steps To Successful Breastfeeding 2Quennie Marie Moreno VillanuevaNo ratings yet
- MaternalDocument5 pagesMaternalStephanie Joy EscalaNo ratings yet
- Doh MCNDocument14 pagesDoh MCNCbrc CebuNo ratings yet
- Cord Prolapse and Cord PresentationDocument21 pagesCord Prolapse and Cord PresentationKwizera virgileNo ratings yet
- Neutralizes The Acidity of The UrethraDocument12 pagesNeutralizes The Acidity of The Urethracresia hidalgoNo ratings yet
- Johana M. AladinDocument14 pagesJohana M. AladinquoraismadelisNo ratings yet