You might also like
- Newton Fund Institutional Links Grants - Application (2018 IL7 - April)Document31 pagesNewton Fund Institutional Links Grants - Application (2018 IL7 - April)Marzuki Panji WijayaNo ratings yet
- StampedeDocument44 pagesStampedeMarzuki Panji WijayaNo ratings yet
- Soal TO AIPKIDocument45 pagesSoal TO AIPKIrosalina80% (5)
- Guias Hemorragia PospartoDocument48 pagesGuias Hemorragia PospartoDai UmqandmcNo ratings yet
- WHO Dengue Hemorrhagic Fever Diagnosis, Treatment, Prevention and Control 1997Document0 pagesWHO Dengue Hemorrhagic Fever Diagnosis, Treatment, Prevention and Control 1997Maryam JamilahNo ratings yet
- Paris PDFDocument44 pagesParis PDFMarzuki Panji WijayaNo ratings yet
- Venous Function and Central Venous Pressure: A Physiologic StoryDocument14 pagesVenous Function and Central Venous Pressure: A Physiologic StoryMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
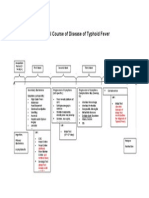
- Natural Course of Disease of Typhoid FeverDocument1 pageNatural Course of Disease of Typhoid FeverMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MPPSC AM Previous Year Question PapersDocument8 pagesMPPSC AM Previous Year Question PapersSETU AWASTHINo ratings yet
- Unit Test in MAPEH 2nd Quarter 18 19Document3 pagesUnit Test in MAPEH 2nd Quarter 18 19Joshua CasemNo ratings yet
- Book For Practical SkillsDocument36 pagesBook For Practical SkillssyhnzNo ratings yet
- Medical Benefit TRFDocument9 pagesMedical Benefit TRFAvijat MondalNo ratings yet
- Learning Activity No. 6Document13 pagesLearning Activity No. 6Jonah MaasinNo ratings yet
- The National Health SituationDocument167 pagesThe National Health SituationCes AriaNo ratings yet
- Daftar Pustaka - 2Document4 pagesDaftar Pustaka - 2YohanesFredyOskieBalsiaNo ratings yet
- Acute PainDocument5 pagesAcute PainEricka MunsayacNo ratings yet
- Saliva ApromisingdiagnostictoolDocument3 pagesSaliva ApromisingdiagnostictoolTitodcNo ratings yet
- Awake Tracheal Intubation 2022Document8 pagesAwake Tracheal Intubation 2022Gloria Stefany Fernandez CabreraNo ratings yet
- PDF Unit Plan For Sem 1 DLDocument17 pagesPDF Unit Plan For Sem 1 DLDiksha chaudharyNo ratings yet
- Child Health Program Oral Health: Guidance DocumentDocument30 pagesChild Health Program Oral Health: Guidance Documentanubhutigupta1404No ratings yet
- FACT SHEET 01-16 For Outpatient Providers and Office ManagersDocument4 pagesFACT SHEET 01-16 For Outpatient Providers and Office ManagersAlan ArmstrongNo ratings yet
- John Williamson and The Terrifying Results of The Medical Practice Information Demonstration ProjectDocument8 pagesJohn Williamson and The Terrifying Results of The Medical Practice Information Demonstration ProjectFrancisco LazoNo ratings yet
- Using Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common PitfallsDocument7 pagesUsing Routine Comparative Data To Assess The Quality of Health Care: Understanding and Avoiding Common Pitfallsujangketul62No ratings yet
- Operating Room Attire JournalDocument1 pageOperating Room Attire JournalMia MabaylanNo ratings yet
- Nutrition For Late Preterm Babies What Should We Know.Document25 pagesNutrition For Late Preterm Babies What Should We Know.IKA UNAIRNo ratings yet
- Kenya ARV Guidelines 2018Document230 pagesKenya ARV Guidelines 2018Felix Wafula MusibiNo ratings yet
- Jadwal September NewDocument20 pagesJadwal September NewWiLly IsmailNo ratings yet
- School of Mount St. Mary, Inc.: Learning Module in Health 10Document25 pagesSchool of Mount St. Mary, Inc.: Learning Module in Health 10rom keroNo ratings yet
- List of Essential Medicine For Adult in Rwanda PDFDocument60 pagesList of Essential Medicine For Adult in Rwanda PDFShandy B100% (1)
- Attracting and Retaining Healthcare StaffDocument9 pagesAttracting and Retaining Healthcare StaffAnonymous MFh19TBNo ratings yet
- Rguhs Thesis Topics in Oral SurgeryDocument6 pagesRguhs Thesis Topics in Oral Surgerysdeaqoikd100% (1)
- 2019 01 07 - Enabling Interoperability For Social and Behavioral Determinants of Health DataDocument69 pages2019 01 07 - Enabling Interoperability For Social and Behavioral Determinants of Health DataDaniel VreemanNo ratings yet
- RhinosinusitisDocument8 pagesRhinosinusitisAyuNo ratings yet
- Ehr Chapter 1 CarterDocument17 pagesEhr Chapter 1 Carterapi-298340093No ratings yet
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-272451466No ratings yet
- SIGN guideline: Risk reduction and management of deliriumDocument2 pagesSIGN guideline: Risk reduction and management of deliriumChika SabaNo ratings yet
- Lesson Plan On CPRDocument3 pagesLesson Plan On CPRanimesh pandaNo ratings yet
- List of Current Aeromedical Examiners as of 2010Document26 pagesList of Current Aeromedical Examiners as of 2010naveenbalaNo ratings yet