You might also like
- VDA Standard - VW PDFDocument152 pagesVDA Standard - VW PDFamezqth2No ratings yet
- Carcinogenesis 2014 SeyfriedDocument13 pagesCarcinogenesis 2014 Seyfriedamezqth2No ratings yet
- Basics of Project ManagementDocument7 pagesBasics of Project ManagementvijaykmjNo ratings yet
- Stealth Persuasion ManifestoDocument28 pagesStealth Persuasion ManifestoSolomon Cosmin Ionut100% (6)
- Handbook of Ericksonian HypnosisDocument82 pagesHandbook of Ericksonian HypnosisMaurício Alejándro Kehrwald100% (2)
- CarpentryDocument549 pagesCarpentryjm50963100% (10)
- 03 Norman 01Document40 pages03 Norman 01yagnyeshNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- Fundamentals of Nursing 1Document6 pagesFundamentals of Nursing 1Ruel M. BersabeNo ratings yet
- ChromagarDocument2 pagesChromagarapi-26429188No ratings yet
- Oral Patho For DR ARA Khan Soft Form PDFDocument43 pagesOral Patho For DR ARA Khan Soft Form PDFreema aslamNo ratings yet
- Sportsdermatology: Skin Disease in AthletesDocument22 pagesSportsdermatology: Skin Disease in Athletesleticia floresNo ratings yet
- Mental Illness Annotated BibliographyDocument8 pagesMental Illness Annotated Bibliographyapi-386396722No ratings yet
- JSA - Doc Job Safety Analysis NewDocument3 pagesJSA - Doc Job Safety Analysis NewKali MuthuNo ratings yet
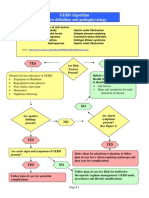
- GERD Algorithm Review Definition and Pathophysiology: NO YESDocument3 pagesGERD Algorithm Review Definition and Pathophysiology: NO YESdianyNo ratings yet
- Rania Nasir 22667 Human Development Assignment 1Document2 pagesRania Nasir 22667 Human Development Assignment 1Rania NasirNo ratings yet
- Obesity What Is Obesity?Document12 pagesObesity What Is Obesity?TABIBI11No ratings yet
- Acog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaDocument4 pagesAcog Practice Bulletin Summary: Gestational Hypertension and PreeclampsiaKevin CasavilcaNo ratings yet
- Acrrm Recalls Latest PDFDocument16 pagesAcrrm Recalls Latest PDFRumana Ali100% (2)
- "Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewDocument6 pages"Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- SuctioningDocument23 pagesSuctioningrnrmmanphd100% (2)
- Numbness: Tyas Mayangputri Hadiana - 10100118204Document7 pagesNumbness: Tyas Mayangputri Hadiana - 10100118204refimaya arlitaNo ratings yet
- Immunization CTP March 2021 4-Per-PageDocument71 pagesImmunization CTP March 2021 4-Per-PageAssal Al JanabiNo ratings yet
- Epidemiology - Exercises. Gaetano MarroneDocument4 pagesEpidemiology - Exercises. Gaetano Marronemillion assefaNo ratings yet
- Roxithromycin TabletDocument13 pagesRoxithromycin Tabletno debedeNo ratings yet
- Understanding Psychosis and SchizophreniaDocument32 pagesUnderstanding Psychosis and SchizophreniaAnonymous zxTFUoqzklNo ratings yet
- Delmar's Pediatric Nursing Care Plans, 3 Edition, Karla L. Luxner, RNC, ND, Pg. 67Document2 pagesDelmar's Pediatric Nursing Care Plans, 3 Edition, Karla L. Luxner, RNC, ND, Pg. 67KMNo ratings yet
- Social Anxiety Disorder 1.editedDocument4 pagesSocial Anxiety Disorder 1.editedmoureenNo ratings yet
- Causes of Pain in The Right Side of The HeadDocument3 pagesCauses of Pain in The Right Side of The HeadUtpal KumarNo ratings yet
- Dr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017Document45 pagesDr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017nanikNo ratings yet
- Lyceum of the Philippines University College of Nursing Drug StudyDocument2 pagesLyceum of the Philippines University College of Nursing Drug Studykaye barrionNo ratings yet
- TofacitinibDocument23 pagesTofacitinibShubham SenguptaNo ratings yet
- A Chiropractor's Treasury of Health SecretsDocument1 pageA Chiropractor's Treasury of Health SecretskenNo ratings yet
- Medicine2 - Myeloproliferative, Lymphoproliferative WorkshopDocument118 pagesMedicine2 - Myeloproliferative, Lymphoproliferative Workshopapi-3762917100% (1)
- Lung Sounds 7Document1 pageLung Sounds 7Kyle LatayanNo ratings yet
- Teaching More About LessDocument3 pagesTeaching More About Lessdutorar hafuNo ratings yet
- Limfoma (Kuliah 3a Ipd III)Document30 pagesLimfoma (Kuliah 3a Ipd III)Rianda Dwi PutraNo ratings yet