You might also like
- Contraception for the Medically Challenging PatientFrom EverandContraception for the Medically Challenging PatientRebecca H. AllenNo ratings yet
- Maternal Hypothyroidism During Pregnancy and The Risk of Pediatric Endocrine Morbidity in The OffspringDocument6 pagesMaternal Hypothyroidism During Pregnancy and The Risk of Pediatric Endocrine Morbidity in The OffspringlananhslssNo ratings yet
- Steroid Antenatal Untuk Pengobatan Imaturitas Paru Janin Setelah 34 Minggu Usia KehamilanDocument23 pagesSteroid Antenatal Untuk Pengobatan Imaturitas Paru Janin Setelah 34 Minggu Usia KehamilanMichaela Vania TanujayaNo ratings yet
- Maternal opioid use linked to birth defectsDocument22 pagesMaternal opioid use linked to birth defectsjulian mukaromNo ratings yet
- Ni Hms 448407Document14 pagesNi Hms 448407Patrick RamosNo ratings yet
- 33873-Article Text-121761-1-10-20170831Document6 pages33873-Article Text-121761-1-10-20170831AnggaNo ratings yet
- In utero pesticide exposure linked to abnormal neonatal reflexesDocument11 pagesIn utero pesticide exposure linked to abnormal neonatal reflexesJorge Ernesto Garcia JimenezNo ratings yet
- A Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenDocument5 pagesA Prospective Cohort Study of Pregnancy Risk Factors and Birth Outcomes in Aboriginal WomenFirman DariyansyahNo ratings yet
- The Effect of Topical Ointment On Neonatal Sepsis in Preterm InfantsDocument4 pagesThe Effect of Topical Ointment On Neonatal Sepsis in Preterm InfantsJill R SendowNo ratings yet
- Journal Reading Diet Sebelum Kehamilan Dan Risiko Hiperemesis GravidarumDocument23 pagesJournal Reading Diet Sebelum Kehamilan Dan Risiko Hiperemesis GravidarumNalendra Tri WidhianartoNo ratings yet
- The Safety of Metoclopramide Use in The First Trimester of PregnancyDocument8 pagesThe Safety of Metoclopramide Use in The First Trimester of PregnancyMentari Cipta SeptikaNo ratings yet
- Antenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane LibraryDocument88 pagesAntenatal Corticosteroids For Accelerating Fetal Lung Maturation For Women at Risk of Preterm Birth - McGoldrick, E - 2020 Cochrane Libraryjavier dauvergneNo ratings yet
- Dyq 030Document10 pagesDyq 030Marlintan Sukma AmbarwatiNo ratings yet
- Antenatal Betamethasone For Women at RiskDocument10 pagesAntenatal Betamethasone For Women at RiskThapakorn JalearnyingNo ratings yet
- Malaria Dan KeguguranDocument23 pagesMalaria Dan Keguguranwoouuw0903No ratings yet
- New PDFDocument6 pagesNew PDFDann RoblezNo ratings yet
- New England Journal Medicine: The ofDocument11 pagesNew England Journal Medicine: The ofDevina Indah PermatasariNo ratings yet
- Jurnal GiziDocument7 pagesJurnal GizijuwitapratiwiNo ratings yet
- Jacka. Maternal and Early Postnatal Nutrition and Mental Health of Offspring by Age 5 Years A Prospective Cohort Study Jacka 2013Document10 pagesJacka. Maternal and Early Postnatal Nutrition and Mental Health of Offspring by Age 5 Years A Prospective Cohort Study Jacka 2013sarbu_mirelaNo ratings yet
- Expectant Versus Aggressive Management in Severe Preeclampsia Remote From TermDocument6 pagesExpectant Versus Aggressive Management in Severe Preeclampsia Remote From Termmiss.JEJENo ratings yet
- Epidemiology of Premature Rupture of Membranes: Factors in Pre-Term BirthsDocument11 pagesEpidemiology of Premature Rupture of Membranes: Factors in Pre-Term BirthsMaulidianaIndahNo ratings yet
- Zapata 2003Document8 pagesZapata 2003Luis RodriguezNo ratings yet
- Chorioamnionitis and Prognosis For Term Infants-13Document5 pagesChorioamnionitis and Prognosis For Term Infants-13ronny29No ratings yet
- Caesarean Section Delivery and The Risk of Allergic Disorders in ChildhoodDocument7 pagesCaesarean Section Delivery and The Risk of Allergic Disorders in ChildhoodRahma Puji LestariNo ratings yet
- Jurnal 3Document10 pagesJurnal 3Dian RianiNo ratings yet
- Pediatrics 2014Document14 pagesPediatrics 2014Randy PrayogoNo ratings yet
- Maternal NutDocument7 pagesMaternal NutShirleuy GonçalvesNo ratings yet
- Maternal Breast Milk Feeding and Length of Treatment in Infants With Neonatal Abstinence SyndromeDocument7 pagesMaternal Breast Milk Feeding and Length of Treatment in Infants With Neonatal Abstinence SyndromeHariCexinkwaeNo ratings yet
- Maternal Smoking During Lactation: Relation To Growth During The First Year of Life in A Dutch Birth CohortDocument10 pagesMaternal Smoking During Lactation: Relation To Growth During The First Year of Life in A Dutch Birth CohortJéssica LacerdaNo ratings yet
- Morning SicknessDocument7 pagesMorning SicknessNovadilah Arifia ShintadewiNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Epidemiology On Asthma Human MilkDocument8 pagesEpidemiology On Asthma Human MilkazaliavirsaNo ratings yet
- Maternal Insulin Resistance and Preeclampsia: ObstetricsDocument6 pagesMaternal Insulin Resistance and Preeclampsia: ObstetricsDiajeng Marta TriajiNo ratings yet
- Pre-Eclampsia Rates in The United States, 1980-2010: Age-Period-Cohort AnalysisDocument9 pagesPre-Eclampsia Rates in The United States, 1980-2010: Age-Period-Cohort AnalysistiyacyntiaNo ratings yet
- Human milk reduces umbilical cord separation timeDocument3 pagesHuman milk reduces umbilical cord separation timeFatma ElzaytNo ratings yet
- Asi 2Document13 pagesAsi 2Fifi FruitasariNo ratings yet
- A Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasDocument7 pagesA Maternal Vegetarian Diet in Pregnancy Is Associated With HypospadiasancoursNo ratings yet
- Neonatal JaundiceDocument5 pagesNeonatal JaundiceKartik KumarasamyNo ratings yet
- Early Growth Delay in Diabetic Relation Psychomotor Development AgeDocument3 pagesEarly Growth Delay in Diabetic Relation Psychomotor Development AgeVasilache DeliaNo ratings yet
- Journal 6Document7 pagesJournal 6Muflih AlghifaryNo ratings yet
- Nejm 2020 1908380Document31 pagesNejm 2020 1908380Dhruvi KansaraNo ratings yet
- Risks of Formula Feeding - A Brief Annotated BibliographyDocument6 pagesRisks of Formula Feeding - A Brief Annotated BibliographyMireiaNo ratings yet
- Protocol Poojitha CompletedDocument15 pagesProtocol Poojitha CompletedPranav SNo ratings yet
- Probiotics in Pregnant Women To Prevent Allergic Disease: A Randomized, Double-Blind TrialDocument8 pagesProbiotics in Pregnant Women To Prevent Allergic Disease: A Randomized, Double-Blind TrialarditaNo ratings yet
- Duration of Breastfeeding and Developmental Milestones During The Latter Half of InfancyDocument6 pagesDuration of Breastfeeding and Developmental Milestones During The Latter Half of InfancyErwin SetiawanNo ratings yet
- Angel Josabad Alonso-CastroWofSDocument23 pagesAngel Josabad Alonso-CastroWofSIara PachêcoNo ratings yet
- Neonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporeDocument7 pagesNeonatal and Obstetric Risk Assessment (NORA) Pregnancy Cohort Study in SingaporePremier PublishersNo ratings yet
- Vita en Lag EstacionDocument11 pagesVita en Lag EstacionCarlos Elio Polo VargasNo ratings yet
- Hernandez, Et Al.Document11 pagesHernandez, Et Al.Yet Barreda BasbasNo ratings yet
- The Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaDocument8 pagesThe Interactive Effect of Prepregnancy Overweight/Obesity and Isolated Maternal Hypothyroxinemia On MacrosomiaAndres GallegosNo ratings yet
- Nejmoa 054244Document12 pagesNejmoa 054244Shintya DewiNo ratings yet
- HHS Public Access: Periconceptional Maternal Fever, Folic Acid Intake, and The Risk For Neural Tube DefectsDocument13 pagesHHS Public Access: Periconceptional Maternal Fever, Folic Acid Intake, and The Risk For Neural Tube DefectsNurul ArdaniNo ratings yet
- Pages 300-331Document31 pagesPages 300-331aptureinc100% (13)
- 'Kangaroo Mother Care' To Prevent Neonatal Deaths Due To Preterm Birth ComplicationsDocument11 pages'Kangaroo Mother Care' To Prevent Neonatal Deaths Due To Preterm Birth ComplicationsLuzdelpilar RcNo ratings yet
- Obesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenDocument10 pagesObesity and The Risk of Newly Diagnosed Asthma in School-Age ChildrenMar LindaNo ratings yet
- Jurnal Obgyn 1aDocument11 pagesJurnal Obgyn 1aAditya Cipta KusumaNo ratings yet
- Omega 3 and Preterm LaborDocument7 pagesOmega 3 and Preterm LaborMeera Al AliNo ratings yet
- Preterm Labour, Antibiotics, and Cerebral Palsy: Scientific Impact Paper No. 33Document8 pagesPreterm Labour, Antibiotics, and Cerebral Palsy: Scientific Impact Paper No. 33oscarNo ratings yet
- Dietary Inflammatory Potential and Risk of Breast Cancer A Population Based Case Control Study in France Cecile StudyDocument25 pagesDietary Inflammatory Potential and Risk of Breast Cancer A Population Based Case Control Study in France Cecile Studymaria.panevayahoo.comNo ratings yet
- Risk Factors Associated With Birth Asphyxia in Phramongkutklao HospitalDocument7 pagesRisk Factors Associated With Birth Asphyxia in Phramongkutklao HospitalIga AmandaNo ratings yet
- Klasifikasi BMI & Profil LipidDocument1 pageKlasifikasi BMI & Profil LipidOkky Rizka SesarinaNo ratings yet
- Melanoma and Other Skin Cancers: What You Need To Know AboutDocument59 pagesMelanoma and Other Skin Cancers: What You Need To Know AboutkikiNo ratings yet
- Omega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenDocument10 pagesOmega-3 Fatty Acid Supplementation During Pregnancy and Respiratory Symptoms in ChildrenJojo RyelciusNo ratings yet
- Breast FeedingDocument11 pagesBreast FeedingJojo RyelciusNo ratings yet
- Clinical ReasoningDocument15 pagesClinical ReasoningJojo RyelciusNo ratings yet
- Abdominal WallDocument75 pagesAbdominal WallJojo RyelciusNo ratings yet
- Get A Good Nights SleepDocument35 pagesGet A Good Nights SleepGeorge Sebastian AntonyNo ratings yet
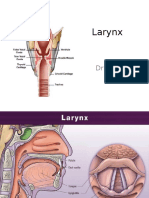
- The Larynx: Structure, Function and Clinical NotesDocument34 pagesThe Larynx: Structure, Function and Clinical NotesJojo Ryelcius100% (1)
- Struktur Clinical ReasoningDocument15 pagesStruktur Clinical ReasoningJojo RyelciusNo ratings yet
- HypoxiaDocument21 pagesHypoxiaJojo RyelciusNo ratings yet
- Stres Cairan Dan SuhuDocument94 pagesStres Cairan Dan SuhuJojo RyelciusNo ratings yet
- Skenario C Blok 10 FixDocument32 pagesSkenario C Blok 10 FixJojo RyelciusNo ratings yet
- Soal Hitungan DosisDocument2 pagesSoal Hitungan DosissabrinaNo ratings yet
- CptchildDocument2 pagesCptchildapi-3709645No ratings yet
- Speech & Language Therapy in Practice, Spring 1998Document32 pagesSpeech & Language Therapy in Practice, Spring 1998Speech & Language Therapy in PracticeNo ratings yet
- Bone Cancer Early Detection, Diagnosis, and StagingDocument22 pagesBone Cancer Early Detection, Diagnosis, and Stagingjinal BhadreshNo ratings yet
- Republic Act No. 7305, Magna Carta of Public Health Workers PDFDocument15 pagesRepublic Act No. 7305, Magna Carta of Public Health Workers PDFSorayah M. Sharief-TabaoNo ratings yet
- Atls Pre Test SolvedDocument18 pagesAtls Pre Test SolvedDr.Mukesh KumarNo ratings yet
- Neurological Assessment 1 - Assessing Level of ConsciousnessDocument1 pageNeurological Assessment 1 - Assessing Level of ConsciousnesskyawswakyawswaNo ratings yet
- Strategi Koping Ibu Dengan Anak Penderita Kanker (Studi Deskriptif Di Komunitas Peduli Anak Kanker Dan Penyakit Kronis Lainnya)Document15 pagesStrategi Koping Ibu Dengan Anak Penderita Kanker (Studi Deskriptif Di Komunitas Peduli Anak Kanker Dan Penyakit Kronis Lainnya)Yan ParirakNo ratings yet
- Bed Side Conference: College of The Holy Spirit of Manila 163 E. Mendiola ST., Manila Telefax: (02) 7347921Document2 pagesBed Side Conference: College of The Holy Spirit of Manila 163 E. Mendiola ST., Manila Telefax: (02) 7347921Jen GarzoNo ratings yet
- The Many Faces of LeadershipDocument6 pagesThe Many Faces of LeadershipbillpaparounisNo ratings yet
- Being Single Vs Being MarriedDocument34 pagesBeing Single Vs Being MarriedPeter MissoleNo ratings yet
- Martha E. Rogers' Theory of Unitary Human BeingsDocument9 pagesMartha E. Rogers' Theory of Unitary Human BeingsCASTRO, ANDREI KARL Z.No ratings yet
- L3 U1 Working As A Close Protection Operative - Dec09Document19 pagesL3 U1 Working As A Close Protection Operative - Dec09twisterxxNo ratings yet
- Epifeed LHFDocument2 pagesEpifeed LHFJoko WiwiNo ratings yet
- Oral Glucose Tolerance TestDocument4 pagesOral Glucose Tolerance TestCyna Jane Yao AlcularNo ratings yet
- 768 - Edited by Yashwardhan Bansal - MEDICAL NEGLIGENCE AND MALPRACTICE A THREAT TO HUMANITY - Shivani UpadhyayDocument12 pages768 - Edited by Yashwardhan Bansal - MEDICAL NEGLIGENCE AND MALPRACTICE A THREAT TO HUMANITY - Shivani UpadhyayANDREW JOSEPHNo ratings yet
- TonsillitisDocument21 pagesTonsillitisWael ShamyNo ratings yet
- Report On Progress of Professional Portfolio - NFDN 1002Document2 pagesReport On Progress of Professional Portfolio - NFDN 1002api-317607382No ratings yet
- Food and Beverage Training RegulationsDocument75 pagesFood and Beverage Training Regulationsfapabear100% (1)
- TRACTIONDocument3 pagesTRACTIONCatherineNo ratings yet
- Willingness To Pay For Improved Health Walk On The Accra-Aburi Mountains Walkway in GhanaDocument9 pagesWillingness To Pay For Improved Health Walk On The Accra-Aburi Mountains Walkway in GhanaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Deviant Behavior Lecture 10 12052023 125827pmDocument10 pagesDeviant Behavior Lecture 10 12052023 125827pmHadia hanif LoyaNo ratings yet
- TechnologiesDocument11 pagesTechnologiesabdelrahmanelsayed368No ratings yet
- Malignant Struma OvariiDocument4 pagesMalignant Struma Ovariixwahyu 108No ratings yet
- Nursing Diagnosis Disturbed Sleep PatternDocument8 pagesNursing Diagnosis Disturbed Sleep Patternmaimai324263100% (2)
- Laguna ProfileDocument23 pagesLaguna ProfileVitaliz GeraldNo ratings yet
- Vitamin D and CalciumDocument33 pagesVitamin D and CalciumAkhmadRoziNo ratings yet
- 03-Ischemic Heart Disease - 2020 OngoingDocument151 pages03-Ischemic Heart Disease - 2020 OngoingDana MohammadNo ratings yet
- Executive Summary: Adult Dental Health Survey 2009Document22 pagesExecutive Summary: Adult Dental Health Survey 2009Musaab SiddiquiNo ratings yet
- BARITEDocument6 pagesBARITEsajad gohariNo ratings yet
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossFrom EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossRating: 4 out of 5 stars4/5 (22)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanFrom EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanRating: 3.5 out of 5 stars3.5/5 (3)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (59)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 2 out of 5 stars2/5 (1)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodFrom EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodRating: 2 out of 5 stars2/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaFrom EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNo ratings yet
- The Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffFrom EverandThe Ultimate Volumetrics Diet: Smart, Simple, Science-Based Strategies for Losing Weight and Keeping It OffNo ratings yet
- Ultrametabolism: The Simple Plan for Automatic Weight LossFrom EverandUltrametabolism: The Simple Plan for Automatic Weight LossRating: 4.5 out of 5 stars4.5/5 (28)
- The Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITFrom EverandThe Toxin Solution: How Hidden Poisons in the Air, Water, Food, and Products We Use Are Destroying Our Health—AND WHAT WE CAN DO TO FIX ITRating: 5 out of 5 stars5/5 (1)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfFrom EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfRating: 5 out of 5 stars5/5 (2)
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossFrom EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossRating: 4.5 out of 5 stars4.5/5 (22)
- Kintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritFrom EverandKintsugi Wellness: The Japanese Art of Nourishing Mind, Body, and SpiritRating: 4.5 out of 5 stars4.5/5 (3)