You might also like
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ECGDocument6 pagesECGMatthew MackeyNo ratings yet
- ECG and ArrhythmiasDocument25 pagesECG and ArrhythmiasRashed ShatnawiNo ratings yet
- Ekg Panum or OsceDocument69 pagesEkg Panum or OsceGladish RindraNo ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Critical Decisions in Emergency and Acute Care ElectrocardiographyFrom EverandCritical Decisions in Emergency and Acute Care ElectrocardiographyNo ratings yet
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- Heart Arrhythmias, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHeart Arrhythmias, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Essential Cardiac Electrophysiology: The Self-Assessment ApproachFrom EverandEssential Cardiac Electrophysiology: The Self-Assessment ApproachNo ratings yet
- EKG Interpretation GuideDocument2 pagesEKG Interpretation GuideFabian Ramirez HincapiéNo ratings yet
- Ecg Made EasyDocument130 pagesEcg Made EasyJOHN ARBIE TATTAO, RN96% (49)
- ECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesDocument102 pagesECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesMustafa A. DawoodNo ratings yet
- Easy ECG GuideDocument17 pagesEasy ECG GuideDr.Chinmay Kulkarni83% (12)
- ECG Interpretation Cheat Sheet PDFDocument1 pageECG Interpretation Cheat Sheet PDFChristine MerrittNo ratings yet
- 11 Steps of ECG - Ali Alnahari PDFDocument16 pages11 Steps of ECG - Ali Alnahari PDFBìnhNo ratings yet
- Cardiac ArrhythmiasDocument4 pagesCardiac Arrhythmiassmurf096No ratings yet
- Sinus Rhythm DisturbancesDocument3 pagesSinus Rhythm DisturbancesMarcus Philip GonzalesNo ratings yet
- ECG Analysis of Coronary CirculationDocument155 pagesECG Analysis of Coronary CirculationDeepika PatelNo ratings yet
- EcgDocument57 pagesEcgenii_ta100% (9)
- Ecg CookbookDocument2 pagesEcg CookbookCalin Popa100% (1)
- ACLS Class Packet PDFDocument9 pagesACLS Class Packet PDFImam GultomNo ratings yet
- EKG RhythmsDocument10 pagesEKG RhythmsQueenNo ratings yet
- Normal Impulse Conduction: Sinoatrial NodeDocument80 pagesNormal Impulse Conduction: Sinoatrial Nodesiusiuwidyanto100% (2)
- ECG: A Noob's Guide to Understanding ElectrocardiographyDocument103 pagesECG: A Noob's Guide to Understanding ElectrocardiographyGhaidaa Sadeq100% (1)
- ECG InterpretationDocument48 pagesECG InterpretationKervayse St.ClairNo ratings yet
- ECG Interpretation - Axis and Conduction AbnormalitiesDocument9 pagesECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- ACLS EKG Rhythms and InterpretationDocument10 pagesACLS EKG Rhythms and Interpretationdonheyzz_02No ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Cardiac Electrophysiology Technician or Electrophysiology TechniDocument2 pagesCardiac Electrophysiology Technician or Electrophysiology Techniapi-78900391No ratings yet
- EKG Rhythms: SVT, Atrial Fibrillation, AV Blocks (39Document10 pagesEKG Rhythms: SVT, Atrial Fibrillation, AV Blocks (39Saidel ElizondoNo ratings yet
- Cardiac Rhythms and Dysrhythmias GuideDocument14 pagesCardiac Rhythms and Dysrhythmias GuideShawn Gaurav Jha100% (1)
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Electrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorDocument77 pagesElectrocardiogram (ECG/EKG) : Jovel Balaba Tangonan InstructorNecky AlbaciteNo ratings yet
- ECGcheatsheet PDFDocument1 pageECGcheatsheet PDFTush RameNo ratings yet
- Cardiac Study Guide PDFDocument11 pagesCardiac Study Guide PDF281175100% (1)
- ECG Master Class-2Document138 pagesECG Master Class-2Shohag ID Center100% (1)
- Guaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsDocument2 pagesGuaranteed To Pass: Exam Tidbits in Easy To Digest, Bite Sized MorselsAmberNo ratings yet
- Common Cardiac Related MedicationsDocument18 pagesCommon Cardiac Related MedicationsTracy100% (2)
- ECG InterpretationDocument1 pageECG InterpretationCecil-An DalanonNo ratings yet
- PR-QRS-TwavesDocument3 pagesPR-QRS-TwavesKelly PrattNo ratings yet
- Read ECGDocument128 pagesRead ECGrehmatakuNo ratings yet
- Ecg Interpretation: Intervals and ComplexesDocument7 pagesEcg Interpretation: Intervals and ComplexesBobet ReñaNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- ECG InterpretationDocument40 pagesECG InterpretationMuhammad BadrushshalihNo ratings yet
- ECG Rhythms GuideDocument6 pagesECG Rhythms GuideJohnildy MatiasNo ratings yet
- Firek - Lipids Lecture Notes PDFDocument3 pagesFirek - Lipids Lecture Notes PDFanishdNo ratings yet
- Krishnan - Pathophysiology of Cardiac Arrhythmias Lecture NotesDocument1 pageKrishnan - Pathophysiology of Cardiac Arrhythmias Lecture NotesanishdNo ratings yet
- Syncope Mnemonic WOMAN 3-2-1 PEDocument3 pagesSyncope Mnemonic WOMAN 3-2-1 PEanishdNo ratings yet
- Brave New World: Managing The Culture of Medicine: UCR Clinical FoundationDocument20 pagesBrave New World: Managing The Culture of Medicine: UCR Clinical FoundationanishdNo ratings yet
- Pericardial TamponadeDocument2 pagesPericardial TamponadeanishdNo ratings yet
- Act As If - Gary BrodskyDocument63 pagesAct As If - Gary Brodskyanishd100% (6)
- Acute Isolated MyocarditisDocument20 pagesAcute Isolated Myocarditismerin sunilNo ratings yet
- EKG Study GuideDocument45 pagesEKG Study GuideBrawner100% (6)
- Death Case Presentation StrokeDocument66 pagesDeath Case Presentation StrokeGrace SihotangNo ratings yet
- Assessment of Comorbidities and Treatment Approaches in Cardiac PatientsDocument8 pagesAssessment of Comorbidities and Treatment Approaches in Cardiac PatientsManeesha KodipelliNo ratings yet
- Table of Contents - Cerebrovascular Disease - Continuum 2020Document2 pagesTable of Contents - Cerebrovascular Disease - Continuum 2020Mariana Hoyos GallegoNo ratings yet
- Myocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPDocument94 pagesMyocardial Diseases: Marvi G. Dulnuan - Niog, MD, FPSPLianne LagayanNo ratings yet
- Cardiac RhythmsDocument12 pagesCardiac RhythmsPete Cobra CobraitiNo ratings yet
- ECG ExamplesDocument25 pagesECG Examplesvinsonpeng26No ratings yet
- Cardiology EmqDocument8 pagesCardiology EmqislamawniNo ratings yet
- Cor Pulmonale Definition, Causes, Symptoms and TreatmentDocument13 pagesCor Pulmonale Definition, Causes, Symptoms and TreatmentRizki JaneldiNo ratings yet
- Lutonix PDFDocument4 pagesLutonix PDFtomNo ratings yet
- ASD Pathophysiology, Signs, Symptoms, and TreatmentDocument1 pageASD Pathophysiology, Signs, Symptoms, and TreatmentMSNo ratings yet
- Pathophysiology of Arteriosclerosis and AtherosclerosisDocument22 pagesPathophysiology of Arteriosclerosis and Atherosclerosisjoyrena ochondraNo ratings yet
- Cardiac Murmurs in Children: FactfileDocument2 pagesCardiac Murmurs in Children: FactfileResya I. NoerNo ratings yet
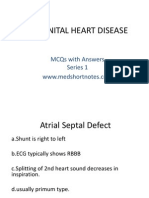
- Congenital Heart Disease Series 1Document9 pagesCongenital Heart Disease Series 1api-216828341No ratings yet
- Murmurs Made Easy Epomedicine 2Document1 pageMurmurs Made Easy Epomedicine 2KC Dela RosaNo ratings yet
- Ashhad's Step 2 CK UW Notes PDFDocument166 pagesAshhad's Step 2 CK UW Notes PDFabNo ratings yet
- Jurnal Coronary Artery FistulaDocument3 pagesJurnal Coronary Artery FistulaRistinyaUnuyNo ratings yet
- Acute Myocardial Infarction Pa Tho Physiology Amp Schematic DiagramDocument6 pagesAcute Myocardial Infarction Pa Tho Physiology Amp Schematic DiagramPeArl PeraltaNo ratings yet
- Inferior Myocardial InfarctionDocument25 pagesInferior Myocardial InfarctionAkbar IskandarNo ratings yet
- EKG Clep TestDocument13 pagesEKG Clep TestElissa LafondNo ratings yet
- Chronic Inappropriate Sinus Tachycardia (Lopera)Document5 pagesChronic Inappropriate Sinus Tachycardia (Lopera)Raymond BernardusNo ratings yet
- Pathophysiology of Myocardial InfarctionDocument2 pagesPathophysiology of Myocardial Infarctionkobe_andre15100% (28)
- Bahir Dar University College of Medicine and Other Health ScienceDocument61 pagesBahir Dar University College of Medicine and Other Health ScienceGizachew AsimareNo ratings yet
- Betarie Anum Almira - RMIK (A) - Praktik KSPK 8Document9 pagesBetarie Anum Almira - RMIK (A) - Praktik KSPK 8Betarie Anum AlmiraNo ratings yet
- Algoritma SVTDocument87 pagesAlgoritma SVTbonne_ameNo ratings yet
- Sick Sinus Syndrome ExplainedDocument12 pagesSick Sinus Syndrome ExplainedlauraNo ratings yet
- Asian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)Document4 pagesAsian Management of Hypertension: Current Status, Home Blood Pressure, and Specific Concerns in Philippines (A Country Report)DORINNE KINDAONo ratings yet
- TplCoverDetailed - Detailed Cover SheetDocument2 pagesTplCoverDetailed - Detailed Cover SheetTara FernandezNo ratings yet
- AMC BLS Training TeamDocument6 pagesAMC BLS Training TeamRajasekhar BandiNo ratings yet