You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Announcement AA BSS1 2017 Press 1a PDFDocument2 pagesAnnouncement AA BSS1 2017 Press 1a PDFAriesta PermatasariNo ratings yet
- Pediatrics 2010 Hinton S37 47Document24 pagesPediatrics 2010 Hinton S37 47Ariesta PermatasariNo ratings yet
- Dapus JurnalDocument1 pageDapus JurnalAriesta PermatasariNo ratings yet
- Jurnal HipotiroidDocument14 pagesJurnal HipotiroidAriesta PermatasariNo ratings yet
- Jurnal HipotiroidDocument14 pagesJurnal HipotiroidAriesta PermatasariNo ratings yet
- 52Document12 pages52Ariesta PermatasariNo ratings yet
- Experimental and Quasi-Experimental Designs: Referensi Kuliah Rancangan Penelitian EksperimentalDocument32 pagesExperimental and Quasi-Experimental Designs: Referensi Kuliah Rancangan Penelitian EksperimentalAriesta PermatasariNo ratings yet
- Pencarian LiteraturDocument20 pagesPencarian LiteraturAriesta PermatasariNo ratings yet
- Referensi Nilai Lab NormalDocument4 pagesReferensi Nilai Lab NormalMuhammad Fikru RizalNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Understated 2200Document3 pagesUnderstated 2200istiakahamed8667No ratings yet
- SSS R3 Contribution Collection List in Excel FormatDocument2 pagesSSS R3 Contribution Collection List in Excel FormatJohn Cando57% (14)
- Salazar vs. Philippines - GuiltyDocument6 pagesSalazar vs. Philippines - Guiltyalwayskeepthefaith8No ratings yet
- Today's Fallen Heroes Wednesday 6 November 1918 (1523)Document31 pagesToday's Fallen Heroes Wednesday 6 November 1918 (1523)MickTierneyNo ratings yet
- Marikina Valley Development Court V Flojo PDFDocument3 pagesMarikina Valley Development Court V Flojo PDFColee StiflerNo ratings yet
- Deed/Waiver of RightsDocument3 pagesDeed/Waiver of RightsButchik Santos100% (4)
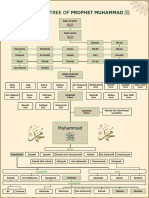
- Family Tree of Prophet MuhammadDocument1 pageFamily Tree of Prophet Muhammadgoogle pro100% (6)
- Remedies Goodman 2013 OutlineDocument42 pagesRemedies Goodman 2013 OutlineCocoNo ratings yet
- Hacking Getting CreditDocument6 pagesHacking Getting Creditsayyed Ayman73% (11)
- Certified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsDocument2 pagesCertified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsSunStar Philippine NewsNo ratings yet
- Social Reform Movements of IndiaDocument5 pagesSocial Reform Movements of IndiaMURALIHARAN KNo ratings yet
- Such A Brutal CrackdownDocument86 pagesSuch A Brutal CrackdownThe Ethiopian AffairNo ratings yet
- Blutms Saas AgreementDocument7 pagesBlutms Saas AgreementAbayomi OlatidoyeNo ratings yet
- Minority Rights in The Constitution of India: Original Research ArticleDocument5 pagesMinority Rights in The Constitution of India: Original Research ArticleSaiby KhanNo ratings yet
- Police LeadershipDocument186 pagesPolice Leadershipsi_imannn100% (1)
- Imposition of Death Penalty - OppositionDocument4 pagesImposition of Death Penalty - OppositionMaeNo ratings yet
- Bezbjednosna Politika Izraela - Andrej BukilicDocument20 pagesBezbjednosna Politika Izraela - Andrej BukilicSeminarski - Maturski RadoviNo ratings yet
- Grievance Redressal Flow ChartDocument1 pageGrievance Redressal Flow ChartAmit PaulNo ratings yet
- Dissertation On Cyber WarfareDocument116 pagesDissertation On Cyber WarfarePaulo DiasNo ratings yet
- MB vs. Reynado DigestDocument2 pagesMB vs. Reynado DigestJewel Ivy Balabag DumapiasNo ratings yet
- Tottel's MiscellanyDocument6 pagesTottel's MiscellanyRoshan EnnackappallilNo ratings yet
- Ephesians 6 Kids CampDocument2 pagesEphesians 6 Kids Campimsevenofnine4No ratings yet
- Annex 1 - Case Digest STATE V SIMPSON, NO. 20160835-CA May 16, 2019 FactsDocument2 pagesAnnex 1 - Case Digest STATE V SIMPSON, NO. 20160835-CA May 16, 2019 FactsmonicatildeNo ratings yet
- Christ King Parish, Gogrial, Wau South Sudan: Proposal On Spiritual Enhancement For ParishionersDocument7 pagesChrist King Parish, Gogrial, Wau South Sudan: Proposal On Spiritual Enhancement For Parishionersroselin sahayamNo ratings yet
- Niña Jewelry Manufacturing of Metal Arts v. Madeline C. MontecilloDocument23 pagesNiña Jewelry Manufacturing of Metal Arts v. Madeline C. MontecilloChatNo ratings yet
- Dissertation Shakespeare S2Document6 pagesDissertation Shakespeare S2Ludmilla BouakkazNo ratings yet
- Maurice Bucaille's InspiringDocument2 pagesMaurice Bucaille's Inspiringsonu24meNo ratings yet
- LEGAL NOTICE NAME DECLARATION AND PROCLAMATION Temple #6Document2 pagesLEGAL NOTICE NAME DECLARATION AND PROCLAMATION Temple #6akenaten7ra7amen0% (1)
- Boarding Pass (BLR-DeL)Document2 pagesBoarding Pass (BLR-DeL)ayush.jainNo ratings yet
- Case Digest Article 28 To 103Document2 pagesCase Digest Article 28 To 103PNP MayoyaoNo ratings yet