You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OMM One LinersDocument21 pagesOMM One LinersBrooklyn Boo-urns100% (1)
- Naim LBM 1-1Document38 pagesNaim LBM 1-1dimasNo ratings yet
- Terapi Cairan LastestDocument31 pagesTerapi Cairan LastestdimasNo ratings yet
- Dismenore: Lampiran 2. Deskripsi Statistik Dan Uji Normalitas Data BMI, Skor VAS, Dan Skor KecemasanDocument14 pagesDismenore: Lampiran 2. Deskripsi Statistik Dan Uji Normalitas Data BMI, Skor VAS, Dan Skor KecemasandimasNo ratings yet
- Journal ReadingDocument1 pageJournal ReadingAdhi NgrNo ratings yet
- Mikrobiologi Penyebab IMS (Dr. Ridha)Document47 pagesMikrobiologi Penyebab IMS (Dr. Ridha)dimasNo ratings yet
- Gibson Et Al (2012) ToyBox ReviewDocument11 pagesGibson Et Al (2012) ToyBox ReviewdimasNo ratings yet
- Tetanus: Maria Banica & Sophie NamDocument19 pagesTetanus: Maria Banica & Sophie NamSuwantin Indra SariNo ratings yet
- Pediatrics 2014 Hambidge E1492 9Document10 pagesPediatrics 2014 Hambidge E1492 9Desrainy InhardiniNo ratings yet
- Jurnal Anak Evidence Based MedicineDocument6 pagesJurnal Anak Evidence Based MedicineMekki Lazir IlhdafNo ratings yet
- GAGAL GINJAL DR - RifqiDocument20 pagesGAGAL GINJAL DR - RifqidimasNo ratings yet
- Abscess Incision and DrainageDocument3 pagesAbscess Incision and DrainageMuhammad Kemal ThoriqNo ratings yet
- Pain Over Speed Bumps Accurately Diagnoses AppendicitisDocument7 pagesPain Over Speed Bumps Accurately Diagnoses AppendicitisdimasNo ratings yet
- Artrocare Cti 2: Additional EquipmentDocument7 pagesArtrocare Cti 2: Additional EquipmentIonela PascarNo ratings yet
- FR and Dislocation of Cervical SpineDocument17 pagesFR and Dislocation of Cervical SpineIreine Soeliongan WaworuntuNo ratings yet
- Lecture Notes - BIOS 1168 Functional Musculoskeletal Anatomy A Revision (Sydney)Document198 pagesLecture Notes - BIOS 1168 Functional Musculoskeletal Anatomy A Revision (Sydney)SK AuNo ratings yet
- Orthopedics MnemonicsDocument8 pagesOrthopedics MnemonicsCristol MyersNo ratings yet
- Spine TraumaDocument52 pagesSpine Traumaapi-26159412100% (1)
- Patologi Tulang Dan SendiDocument79 pagesPatologi Tulang Dan SendiDio Reynaldi SusantoNo ratings yet
- Interlocking NailingDocument211 pagesInterlocking NailingJulio EspinozaNo ratings yet
- Skeletal System Word DocumentDocument4 pagesSkeletal System Word DocumentleesclassroomNo ratings yet
- Journal Reading-DM Hennie Bertha O-16711067Document56 pagesJournal Reading-DM Hennie Bertha O-16711067Suwandi BaskoroNo ratings yet
- The Endoskeleton of Birds.Document29 pagesThe Endoskeleton of Birds.Ian LasarianoNo ratings yet
- Anatomy and PhysiologyDocument2 pagesAnatomy and PhysiologyRagiel AzcarragaNo ratings yet
- Skeletal Lab ReportDocument5 pagesSkeletal Lab Reportapi-296590009No ratings yet
- Jenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Document5 pagesJenisie Pasigan - Ch. 8-2 - Skeletal System Notes Packet (Part II)Jenisie PasiganNo ratings yet
- MDS AnatomyDocument25 pagesMDS AnatomydrpnnreddyNo ratings yet
- 002 Musculoskeletal-Waleed-AltalabiDocument44 pages002 Musculoskeletal-Waleed-Altalabiمحمدعبدالخالق العلوانيNo ratings yet
- Hand Radiology ABC PDFDocument4 pagesHand Radiology ABC PDFJames Carvajal AcostaNo ratings yet
- Bones of the Axial Skeleton ExplainedDocument4 pagesBones of the Axial Skeleton ExplainedJasminKate SutacioNo ratings yet
- Obstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineDocument67 pagesObstetric Anatomy: Professor of Obstetrics & Gynecology Ain Shams Faculty of MedicineJoan LuisNo ratings yet
- Bone FractureDocument23 pagesBone FractureClifford GulfanNo ratings yet
- Joint Disease and Developmental DisordersDocument42 pagesJoint Disease and Developmental DisordersSamuel InbarajaNo ratings yet
- Bones and LimbsDocument147 pagesBones and LimbsDana IonescuNo ratings yet
- Grand PracsDocument13 pagesGrand PracsChristian Allen SibalaNo ratings yet
- MAXILLADocument21 pagesMAXILLACamille MagdirilaNo ratings yet
- Stefanie Veraa 5f22ee8ce4b19Document188 pagesStefanie Veraa 5f22ee8ce4b19JoséMiguelAvendañoNo ratings yet
- Hindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)Document4 pagesHindfoot Valgus: AP Talocalcaneal Angle (Kite's Angle)JoaoNo ratings yet
- DR - Khaldoun Osteoid Osteoma Case ReportDocument4 pagesDR - Khaldoun Osteoid Osteoma Case ReportcyberjaleelNo ratings yet
- Knes 360 - 2021 Spring SyllabusDocument5 pagesKnes 360 - 2021 Spring SyllabusAbdullah KhanNo ratings yet
- Bones of the Upper LimbDocument31 pagesBones of the Upper Limbragnarok meroNo ratings yet
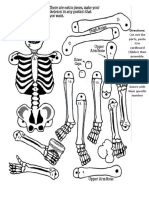
- Assemble the Moving SkeletonDocument1 pageAssemble the Moving SkeletonChristopher UrbinoNo ratings yet