You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Clinical ExemplarDocument4 pagesClinical Exemplarapi-302664008No ratings yet
- Minnesota CertificateDocument1 pageMinnesota Certificateapi-302664008No ratings yet
- Ihi Certificate - Introduction To Population HealtDocument1 pageIhi Certificate - Introduction To Population Healtapi-302664008No ratings yet
- Ihi Certificate - Introduction To Population HealtDocument1 pageIhi Certificate - Introduction To Population Healtapi-302664008No ratings yet
- Pane CertDocument1 pagePane Certapi-302664008No ratings yet
- Pharm Smoking Cessation-1Document1 pagePharm Smoking Cessation-1api-302664008No ratings yet
- Motivational Smoking Cessation-1Document1 pageMotivational Smoking Cessation-1api-302664008No ratings yet
- FemaDocument1 pageFemaapi-302664008No ratings yet
- PatDocument24 pagesPatapi-302664008No ratings yet
- Pat Med Surg IDocument22 pagesPat Med Surg Iapi-302664008No ratings yet
- Medical Errors CertificateDocument1 pageMedical Errors Certificateapi-302664008No ratings yet
- Fundys Nutrition CHFDocument4 pagesFundys Nutrition CHFapi-302664008No ratings yet
- Projectnurse UsfDocument19 pagesProjectnurse Usfapi-302664008No ratings yet
- CapstoneDocument15 pagesCapstoneapi-302664008No ratings yet
- Discharge Planning ProjectDocument8 pagesDischarge Planning Projectapi-302664008No ratings yet
- Personal Professional GoalsDocument2 pagesPersonal Professional Goalsapi-302664008No ratings yet
- Nurse Cover LetterDocument1 pageNurse Cover Letterapi-302664008No ratings yet
- Korovich Resume WeeblyDocument2 pagesKorovich Resume Weeblyapi-302664008No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Maxillary Major ConnectorsDocument20 pagesMaxillary Major ConnectorsRohan GroverNo ratings yet
- Multiple Atrophy System (MSA) Trust Caregiver's GuideDocument11 pagesMultiple Atrophy System (MSA) Trust Caregiver's GuideThe Multiple System Atrophy CoalitionNo ratings yet
- Bisecting and Parelling TechniqueDocument32 pagesBisecting and Parelling TechniqueArka Saha100% (1)
- Overview of Child Health NursingDocument22 pagesOverview of Child Health NursingnatalieshirleyNo ratings yet
- Biopsychosocial AssessmentDocument8 pagesBiopsychosocial AssessmentAnn OgoloNo ratings yet
- Resume Hi Bar A ZackDocument1 pageResume Hi Bar A ZackAsma AlkuwariNo ratings yet
- Lung Contusion & Traumatic AsphyxiaDocument17 pagesLung Contusion & Traumatic AsphyxiaLady KeshiaNo ratings yet
- Anxiety Disorders in ChildrenDocument3 pagesAnxiety Disorders in ChildrenooiseowwweiNo ratings yet
- Presentasi Pit Perbani 2000Document16 pagesPresentasi Pit Perbani 2000Meta ParamitaNo ratings yet
- Benefits of Medical Expert SystemsDocument27 pagesBenefits of Medical Expert Systemsrobertxxx100% (1)
- Test - 10 Root (Radicular) CystsDocument5 pagesTest - 10 Root (Radicular) CystsIsak ShatikaNo ratings yet
- Bathing An Adult ClientDocument8 pagesBathing An Adult ClientXoisagesNo ratings yet
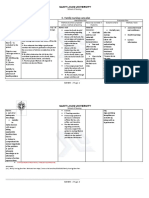
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Baystate Med CTR Rapid Response Team Recordwith SBARDocument3 pagesBaystate Med CTR Rapid Response Team Recordwith SBARDanishyana DhiwaneoNo ratings yet
- ABC of DiabetesDocument111 pagesABC of DiabetesCandy E Ri ViNo ratings yet
- Neonatal ShockDocument50 pagesNeonatal ShockBenazir Nabilla RojwaaNo ratings yet
- Fibrous Dysplasia of The Anterior Mandible A Rare HDocument6 pagesFibrous Dysplasia of The Anterior Mandible A Rare HyesikaichaaNo ratings yet
- Zolendronat NEJMDocument11 pagesZolendronat NEJMnoveldycb89No ratings yet
- NURS FPX 6016 Assessment 1 Adverse Event or Near-Miss AnalysisDocument6 pagesNURS FPX 6016 Assessment 1 Adverse Event or Near-Miss Analysisjoohnsmith070No ratings yet
- Group MediclaimDocument21 pagesGroup MediclaimAishwarya Deepak ChintalapatiNo ratings yet
- Applying The Four Principles of BioEthicsDocument3 pagesApplying The Four Principles of BioEthicsAurelia Pinder100% (1)
- Diagnosis Management of HypertensionDocument23 pagesDiagnosis Management of Hypertensionarahman168No ratings yet
- The Facts About Fillings: Dental Materials - Advantages & Disadvantages Porcelain Fused To Metal Gold AlloyDocument4 pagesThe Facts About Fillings: Dental Materials - Advantages & Disadvantages Porcelain Fused To Metal Gold AlloyIsak Isak IsakNo ratings yet
- RamiprilDocument3 pagesRamiprilapi-3797941No ratings yet
- Ketoconazole: SampleDocument7 pagesKetoconazole: SampleJuan PerezNo ratings yet
- Basic Implant SurgeryDocument7 pagesBasic Implant SurgeryDr.Ankur Gupta100% (1)
- Worn DentitionDocument8 pagesWorn DentitionHassan MoussaouiNo ratings yet
- Quick Selection of Chinese Herbal Formulas Based On Clinical ConditionsDocument0 pagesQuick Selection of Chinese Herbal Formulas Based On Clinical Conditionsharbor100% (1)
- Surgical Treatment of Talus Fractures PDFDocument9 pagesSurgical Treatment of Talus Fractures PDFumesh sarojNo ratings yet
- Alternativas A TotalesDocument12 pagesAlternativas A TotalesJuan Jose Stuven RodriguezNo ratings yet