You might also like
- Toxic Anterior Segment SyndromeDocument13 pagesToxic Anterior Segment SyndromePrathibha M ChachadiNo ratings yet
- MSK CasesDocument331 pagesMSK CasesRadio Resident100% (6)
- Olive Leaf ExtractDocument9 pagesOlive Leaf ExtractCristina100% (1)
- RetinoblastomaDocument24 pagesRetinoblastomaMiguel Carlos Navarro Tacderan100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- NCPDocument22 pagesNCPMaricris S. Sampang100% (1)
- Nursing Care PlanDocument10 pagesNursing Care PlanGinel Laquiores100% (1)
- Nursing Care Plan Problem: Difficulty of BreathingDocument5 pagesNursing Care Plan Problem: Difficulty of BreathingIvan Louise Fajardo ManiquizNo ratings yet
- Blood Banking Course BookDocument2 pagesBlood Banking Course BookShukr Wesman BlbasNo ratings yet
- Cap NCPDocument6 pagesCap NCPMarlo Parayno100% (2)
- GRP4 - Ppt-Diabetes InsipidusDocument12 pagesGRP4 - Ppt-Diabetes InsipidusNicole Villanueva, BSN - Level 3A100% (2)
- Care of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryDocument13 pagesCare of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryRazel Kinette AzotesNo ratings yet
- Postpartum Visit by Healthcare WorkersDocument6 pagesPostpartum Visit by Healthcare WorkersStephy Sojan100% (1)
- Oxygen Terapi Dan PrinsipelDocument16 pagesOxygen Terapi Dan PrinsipelAmrita KaurNo ratings yet
- Fluorosis: Fluoride Toxicity: Patient Management & MonitoringDocument24 pagesFluorosis: Fluoride Toxicity: Patient Management & MonitoringdrjriNo ratings yet
- Effectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesDocument3 pagesEffectiveness of Planned Teaching Programme On Knowledge Regarding Needle Stick Injury Among The Staff NursesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Research ProposalDocument22 pagesResearch ProposalKapil LakhwaraNo ratings yet
- NCPGDMDocument8 pagesNCPGDMChristopher LontocNo ratings yet
- Nursing Care PlansDocument6 pagesNursing Care PlansRoxanne MariÑas Delvo0% (1)
- Assessment Diagnosis Planning Intrvention Rationale EvaluationDocument1 pageAssessment Diagnosis Planning Intrvention Rationale EvaluationMar OrdanzaNo ratings yet
- Assessment Nursing Diagnosis Planning Interventions EvaluationsDocument4 pagesAssessment Nursing Diagnosis Planning Interventions EvaluationsAjay SupanNo ratings yet
- Tracheostomy CareDocument40 pagesTracheostomy CareSreelekhaNo ratings yet
- Drug Presentation On AminophyllineDocument10 pagesDrug Presentation On Aminophyllineelisha immanuelNo ratings yet
- Nicu Lesson PlanDocument11 pagesNicu Lesson PlanSAYMABANUNo ratings yet
- 4 Flow Chart PretermDocument4 pages4 Flow Chart PretermYeni PuspitaNo ratings yet
- C12 P13 TubectomyDocument24 pagesC12 P13 TubectomyRaviKurleNo ratings yet
- UNFPADocument17 pagesUNFPAshipra arora50% (2)
- Cataract: Case Presentation - M.E.T.H.O.DDocument7 pagesCataract: Case Presentation - M.E.T.H.O.DKismet SummonsNo ratings yet
- Pregnancy Induced Hypertension Nursing Diagnosis NANDADocument9 pagesPregnancy Induced Hypertension Nursing Diagnosis NANDASanal S SalimNo ratings yet
- Different BandagingDocument2 pagesDifferent BandagingMarc LimNo ratings yet
- Dengue-WPS OfficeDocument20 pagesDengue-WPS OfficeAnnamalai MNo ratings yet
- HyperthermiaDocument2 pagesHyperthermiaLeolene Grace BautistaNo ratings yet
- Activity Intolerance R/T Increased Energy Demands Due To Disease Condition and Increased Fetal Nutrient UptakeDocument8 pagesActivity Intolerance R/T Increased Energy Demands Due To Disease Condition and Increased Fetal Nutrient UptakeAbdelmar SusulanNo ratings yet
- SEMINAR On New FilariaDocument50 pagesSEMINAR On New FilariaArun JvNo ratings yet
- Drug Study MetforminDocument2 pagesDrug Study MetforminLilly Patterson0% (1)
- Assessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentDocument7 pagesAssessment Nursing Diagnosis Outcome Identification Planning Nursing Intervention Evaluation IndependentQueenie Silva100% (1)
- Osteomalacia Care Plan/OthersDocument11 pagesOsteomalacia Care Plan/OthersJill Jackson, RNNo ratings yet
- Nursing Care Plan D-CDocument2 pagesNursing Care Plan D-CGian MonillaNo ratings yet
- Nursing Care Plan Nephrotic SyndromeDocument2 pagesNursing Care Plan Nephrotic SyndromeJames Pachejo100% (1)
- Clinical Learning ContractDocument3 pagesClinical Learning ContractKaragire vedasteNo ratings yet
- Nursing Care Plan On: Ca OvaryDocument13 pagesNursing Care Plan On: Ca Ovaryvaishali TayadeNo ratings yet
- SUBDocument18 pagesSUBArun KumarNo ratings yet
- Diphtheria SlideDocument11 pagesDiphtheria Slideandre andreNo ratings yet
- NCLFNP - Mr. Robert McClelland CaseDocument4 pagesNCLFNP - Mr. Robert McClelland CaseAiresh Lamao50% (2)
- Cholera N C P BY BHERU LALDocument2 pagesCholera N C P BY BHERU LALBheru LalNo ratings yet
- PEDIA CASE 3 FinalDocument9 pagesPEDIA CASE 3 FinalXandra BnnNo ratings yet
- Nursing Care of Head InjuryDocument1 pageNursing Care of Head InjuryRaveen mayiNo ratings yet
- of Abg ResearchDocument20 pagesof Abg ResearchKhirabdhi Tanaya Sahu100% (1)
- Nursing Careplan - Rectal CancerDocument5 pagesNursing Careplan - Rectal CancerdrugcardrefNo ratings yet
- Specialized Community Health NursingDocument45 pagesSpecialized Community Health NursingdaveNo ratings yet
- NCP PPHDocument2 pagesNCP PPHMark Joseph Christian100% (1)
- Education Sub Cutaneous Injection Lesson PlanDocument12 pagesEducation Sub Cutaneous Injection Lesson Planamrutha h s100% (1)
- Case Report Chronic OsteomyelitisDocument34 pagesCase Report Chronic OsteomyelitisNardine Roslan100% (1)
- ChemotherapyDocument11 pagesChemotherapyRekha G.No ratings yet
- Mo Handbook Fbimnci Apr 18, 2019Document296 pagesMo Handbook Fbimnci Apr 18, 2019Prakash Thakulla100% (1)
- Nursing Care PlanDocument6 pagesNursing Care Plankreny1050% (2)
- NCPDocument2 pagesNCPJamaica SaranquinNo ratings yet
- Translational Research: Generating Evidence For PracticeDocument24 pagesTranslational Research: Generating Evidence For Practicebeer_ettaaNo ratings yet
- Care Plan For GastrectomyDocument16 pagesCare Plan For GastrectomyPriyal ParikhNo ratings yet
- Cholecystectomy Nursing Care Plan: Risk For InfectionDocument1 pageCholecystectomy Nursing Care Plan: Risk For InfectionBesael BaccolNo ratings yet
- JDM Care PlanDocument5 pagesJDM Care PlangopscharanNo ratings yet
- Introduction To Community Health and Environmental Sanitation PDFDocument44 pagesIntroduction To Community Health and Environmental Sanitation PDFKaty SanchezNo ratings yet
- Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument8 pagesWhich It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- Nursing Care Plan - Airway ClearanceDocument3 pagesNursing Care Plan - Airway Clearance3015 MOHD NAJMI BIN ABDULLAHNo ratings yet
- And Release of Pancreatic Enzyme: Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToDocument15 pagesAnd Release of Pancreatic Enzyme: Which It Is A Process Whereby Pancreatic Enzymes Destroy Its Own Tissue Leading ToAriane-Gay Cristobal DuranNo ratings yet
- Drug Dosage Mechanism of Action Specific Indication Contraindicati ON Adverse Effect Nursing PrecautionDocument11 pagesDrug Dosage Mechanism of Action Specific Indication Contraindicati ON Adverse Effect Nursing PrecautionIzabela UyNo ratings yet
- Australian Disaster TriageDocument6 pagesAustralian Disaster TriageIzabela UyNo ratings yet
- Drug Dosage Mechanism of Action Specific Indicatio N Contraindicat ION Adverse Effect Nursing PrecautionDocument14 pagesDrug Dosage Mechanism of Action Specific Indicatio N Contraindicat ION Adverse Effect Nursing PrecautionIzabela UyNo ratings yet
- Coffee ConsumptionDocument6 pagesCoffee ConsumptionIzabela Uy0% (1)
- NewsCap Coffee, Tea, or Diabetes .11Document1 pageNewsCap Coffee, Tea, or Diabetes .11Izabela UyNo ratings yet
- Coffee ConsumptionDocument6 pagesCoffee ConsumptionIzabela Uy0% (1)
- Nature's Pathways Nov 2013 Issue - Northeast WI EditionDocument96 pagesNature's Pathways Nov 2013 Issue - Northeast WI EditionNature's PathwaysNo ratings yet
- Esophageal Cancer PDFDocument16 pagesEsophageal Cancer PDFAJ AYNo ratings yet
- Javma-Javma 21 04 0213Document5 pagesJavma-Javma 21 04 0213Black manNo ratings yet
- Mufrodat Fil MusytasyfaDocument3 pagesMufrodat Fil MusytasyfaNenazNaziahNo ratings yet
- Vaastu and CancerDocument2 pagesVaastu and CancervivekpatelbiiNo ratings yet
- Association Between Work-Related Stress and Coronary Heart Disease: A Review of Prospective Studies Through The Job Strain, Effort-Reward Balance, and Organizational Justice ModelsDocument15 pagesAssociation Between Work-Related Stress and Coronary Heart Disease: A Review of Prospective Studies Through The Job Strain, Effort-Reward Balance, and Organizational Justice ModelsthomasNo ratings yet
- Post Doc Proposal PDFDocument9 pagesPost Doc Proposal PDFMaqsood RehmanNo ratings yet
- The Prevalence of Severe Malaria in Children Below Five Years of Age at Hoima Regional Referral Hospital, Hoima CityDocument9 pagesThe Prevalence of Severe Malaria in Children Below Five Years of Age at Hoima Regional Referral Hospital, Hoima CityKIU PUBLICATION AND EXTENSIONNo ratings yet
- Granulomatous Diseases Affecting Oral Cavity: A ReviewDocument7 pagesGranulomatous Diseases Affecting Oral Cavity: A ReviewVikrant VazeNo ratings yet
- Review Article: Ridge Preservation Procedures After Tooth Extractions: A Systematic ReviewDocument8 pagesReview Article: Ridge Preservation Procedures After Tooth Extractions: A Systematic ReviewIka KusumawatiNo ratings yet
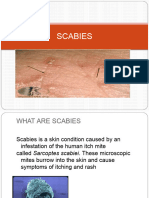
- ScabiesDocument14 pagesScabiessyemiNo ratings yet
- Surgery (EACTS)Document116 pagesSurgery (EACTS)Sergio Vidal Mamani VillarrealNo ratings yet
- MLD - Chapter 5Document8 pagesMLD - Chapter 5ann. ssNo ratings yet
- AI and Health CareDocument4 pagesAI and Health Careaastha.tiwariNo ratings yet
- Community - Based NursingDocument16 pagesCommunity - Based NursingManu CvNo ratings yet
- AsdsDocument5 pagesAsdsGerald MasagandaNo ratings yet
- Immunological DisordersDocument78 pagesImmunological DisordersAshwathy ThomasNo ratings yet
- Body Develop Fever After An InfectionDocument10 pagesBody Develop Fever After An InfectionAfiq_Raimi_4815No ratings yet
- Chikungunya Fever - WHO FactSheetDocument2 pagesChikungunya Fever - WHO FactSheetDr.SagindarNo ratings yet
- Neoplasia Outline Notes - PathologyDocument4 pagesNeoplasia Outline Notes - Pathologykep1313No ratings yet
- Public Health Approaches To Malaria: Source: National Library of MedicineDocument24 pagesPublic Health Approaches To Malaria: Source: National Library of MedicineRahmalia Fitri RosaNo ratings yet
- Pathophysiology - PyelonephritisDocument2 pagesPathophysiology - PyelonephritisFrancis Kevin Sagudo92% (13)
- Pharmacotherapy of HypertensionDocument52 pagesPharmacotherapy of HypertensionDrVinod Kumar Goud VemulaNo ratings yet
- The Top 10 Dysmorphic Syndromes: Keys To Diagnosis/What's HotDocument60 pagesThe Top 10 Dysmorphic Syndromes: Keys To Diagnosis/What's HotTom ChanNo ratings yet
- Musni Theo Roi Ncm116a - DS MedwardDocument2 pagesMusni Theo Roi Ncm116a - DS Medwardjovert davidNo ratings yet