You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Transformation TenDocument28 pagesThe Transformation TenRob AtkinNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Turmeric For Your Thyroid and HashimotoDocument34 pagesTurmeric For Your Thyroid and Hashimotoalbinuta100% (1)
- Hair Loss Chart: Yourself, Then You Might Not Need ThisDocument46 pagesHair Loss Chart: Yourself, Then You Might Not Need ThisVinayak KhambeteNo ratings yet
- Fundamentals of NutritionDocument55 pagesFundamentals of NutritionIhsan BadshaNo ratings yet
- Nutrients: Methylsulfonylmethane: Applications and Safety of A Novel Dietary SupplementDocument21 pagesNutrients: Methylsulfonylmethane: Applications and Safety of A Novel Dietary SupplementRoberto CarvalhoNo ratings yet
- Ferrous Sulfate Drug StudyDocument1 pageFerrous Sulfate Drug Studymilkv80% (10)
- Development of Carrots Pastillas with MalunggayDocument12 pagesDevelopment of Carrots Pastillas with MalunggayKemp Moore100% (6)
- Abdominal TraumaDocument47 pagesAbdominal TraumaWidya Rahayu100% (1)
- HaisDocument1 pageHaisFazax FazaNo ratings yet
- Case Report OmskDocument34 pagesCase Report OmskFazax FazaNo ratings yet
- Osteoarthritis Report SummaryDocument30 pagesOsteoarthritis Report SummaryFazax FazaNo ratings yet
- Ttest AnovaDocument13 pagesTtest AnovaRizqidio LarisoNo ratings yet
- Diabetes and HerbsDocument132 pagesDiabetes and HerbsAjmal KhanNo ratings yet
- The Keys to Progressive Resistance TrainingDocument8 pagesThe Keys to Progressive Resistance TrainingTomrules100% (1)
- Anthropometry 130824161551 Phpapp02Document48 pagesAnthropometry 130824161551 Phpapp02cuckoo1234No ratings yet
- Um 0sm00396 m1 Kinesispersonal Printing - PDF AllDocument128 pagesUm 0sm00396 m1 Kinesispersonal Printing - PDF AllDaniel GarnicaNo ratings yet
- The History and Manufacturing Process of Pasta Around the WorldDocument6 pagesThe History and Manufacturing Process of Pasta Around the WorldSuman Taya JainNo ratings yet
- AcenocoumarolDocument2 pagesAcenocoumarolSpircă Ioana-AndreeaNo ratings yet
- BrainBike: Exercise For The Brain and The Body by Dan Lawler, Ph.D.Document2 pagesBrainBike: Exercise For The Brain and The Body by Dan Lawler, Ph.D.exergamefitnessNo ratings yet
- Dates TypesDocument17 pagesDates TypesMetzelderNo ratings yet
- PhenylDocument3 pagesPhenylVince PaelmoNo ratings yet
- (50-59) Growth Performance of Broiler Chickens Fed Diets Containing Partially Cooked Sweet Potato MealDocument11 pages(50-59) Growth Performance of Broiler Chickens Fed Diets Containing Partially Cooked Sweet Potato MealAlexander DeckerNo ratings yet
- Causes, Symptoms and Tests for High Vitamin D LevelsDocument3 pagesCauses, Symptoms and Tests for High Vitamin D LevelsbhatambarekarNo ratings yet
- Bio MoleculesDocument45 pagesBio MoleculesAngelica MartinNo ratings yet
- Nursing Care of Patients With Diabetes MellitusDocument19 pagesNursing Care of Patients With Diabetes MellitusZyad DaghririNo ratings yet
- HakdoggggDocument2 pagesHakdoggggHarry Venzon JaboliNo ratings yet
- Honey - Prophet's Guidance Regarding The Usuage of ItDocument3 pagesHoney - Prophet's Guidance Regarding The Usuage of ItAsfaqul HaqueNo ratings yet
- Consumer Perception and The Role of Science in The Meat IndustryDocument13 pagesConsumer Perception and The Role of Science in The Meat IndustryAriel IbarraNo ratings yet
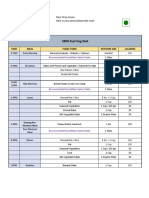
- 2800 Kcal Veg Diet: Time Meal Food Items Portion Size CaloriesDocument2 pages2800 Kcal Veg Diet: Time Meal Food Items Portion Size CaloriesSiraj AnsariNo ratings yet
- Bird Digestive System OverviewDocument24 pagesBird Digestive System OverviewWiwit Yuliyanti LestariNo ratings yet
- CKD Nutrition/Dietetics WorksheetsDocument12 pagesCKD Nutrition/Dietetics WorksheetsSyeda Zainab AbbasNo ratings yet
- Low-Calorie Sweetener Allulose ExplainedDocument1 pageLow-Calorie Sweetener Allulose ExplainedJagadeesh KumarNo ratings yet
- Marketing Plan For Dairy State Whey Docx2 2Document20 pagesMarketing Plan For Dairy State Whey Docx2 2api-303144920No ratings yet
- 3rd Year Precept Pedia Case 4 HydroceleDocument4 pages3rd Year Precept Pedia Case 4 Hydrocelekristel_nicole18yaho100% (1)
- Nutrition Essentials for Strong BonesDocument30 pagesNutrition Essentials for Strong BonesazwararifkiNo ratings yet