You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Parade OK 3 07 June 2017Document9 pagesParade OK 3 07 June 2017Dini NanamiNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Rekap Pasien Bedah Digestive Selasa, 08 November 2016: Nama Dokter MudaDocument6 pagesRekap Pasien Bedah Digestive Selasa, 08 November 2016: Nama Dokter MudaDini NanamiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Soal Uts Lp3iDocument1 pageSoal Uts Lp3iDini NanamiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Art:10.1007/s00431 007 0419 XDocument8 pagesArt:10.1007/s00431 007 0419 XDini NanamiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Rekap Pasien Bedah Digestive Minggu, 13 November 2016: Nama Dokter MudaDocument6 pagesRekap Pasien Bedah Digestive Minggu, 13 November 2016: Nama Dokter MudaDini NanamiNo ratings yet
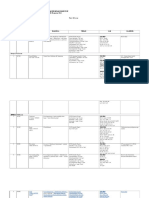
- 190 Chronic Diarrhea: EtiologyDocument14 pages190 Chronic Diarrhea: EtiologyDini NanamiNo ratings yet
- Functional Diarrhea in Toddlers (Chronic Nonspeci Fi C Diarrhea)Document4 pagesFunctional Diarrhea in Toddlers (Chronic Nonspeci Fi C Diarrhea)Dini NanamiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Ruptured Cerebral Aneurysms: PerspectiveDocument4 pagesRuptured Cerebral Aneurysms: PerspectiveDini NanamiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Snow ASR 1980Document16 pagesSnow ASR 1980Dini Nanami100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Crosstabs Umur Mekanisme Koping: CrosstabDocument10 pagesCrosstabs Umur Mekanisme Koping: CrosstabDini NanamiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- NPH BookletDocument41 pagesNPH BookletDini NanamiNo ratings yet
- Diagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDocument11 pagesDiagnosis of Idiopathic Normal Pressure Hydrocephalus Is Supported by MRI-based Scheme: A Prospective Cohort StudyDini NanamiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Canadian Diabetes Clinical Guidelines 2008Document215 pagesCanadian Diabetes Clinical Guidelines 2008FelipeOrtiz100% (4)
- GBS Source 1Document4 pagesGBS Source 1PJHG50% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Conducting A Nurse Consultation: ClinicalDocument6 pagesConducting A Nurse Consultation: ClinicalAlif Akbar HasyimiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- About DysphoriaDocument5 pagesAbout DysphoriaCarolina GómezNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Cholelithiasis Case 1Document21 pagesCholelithiasis Case 1Arvin F. LansangNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- VTE Risk AssessmentDocument2 pagesVTE Risk AssessmentpriyopanjiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ATO - Compassionate - Release - of - SuperannuationDocument5 pagesATO - Compassionate - Release - of - SuperannuationBen RamalliNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- List of PG Students' Passed in May 2019 ExaminiationDocument4 pagesList of PG Students' Passed in May 2019 Examiniationyogesh kumarNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Clinical Handbook of Couple TherapyDocument2 pagesClinical Handbook of Couple TherapyLaura AndreiNo ratings yet
- Report ViewerDocument1 pageReport Viewervoldemort killerNo ratings yet
- Integrative Final DraftDocument16 pagesIntegrative Final Draftapi-532928007No ratings yet
- FIT HW - Module 2Document34 pagesFIT HW - Module 2Ivan Louis C. ARNOBITNo ratings yet
- ESHRE Guideline EndometriosisDocument27 pagesESHRE Guideline EndometriosisRodiani MoekroniNo ratings yet
- LaryngoscopeDocument97 pagesLaryngoscopeMohammed NaserNo ratings yet
- Fundamentals of NursingDocument44 pagesFundamentals of Nursingtheglobalnursing100% (2)
- Piperacillin TazobactamDocument2 pagesPiperacillin TazobactamAnonymous43% (7)
- Sleep Disorders in Children and Adolescents: Deepti Shenoi MDDocument50 pagesSleep Disorders in Children and Adolescents: Deepti Shenoi MDCitra Sukri Sugesti100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- VS TL - Protein - L1 29261 2303 3Document7 pagesVS TL - Protein - L1 29261 2303 3Hadi BitarNo ratings yet
- Paediatrics: Final Exam National Board of Examinations December 2011Document4 pagesPaediatrics: Final Exam National Board of Examinations December 2011AlolikaNo ratings yet
- Hypertency Emergency Acute PDFDocument12 pagesHypertency Emergency Acute PDFmasdika09No ratings yet
- 1-Collection, Storage and Transportataion of MicrobiologicalDocument49 pages1-Collection, Storage and Transportataion of MicrobiologicalSummi NizNo ratings yet
- Retinal Drawing: A Lost Art of MedicineDocument2 pagesRetinal Drawing: A Lost Art of MedicineManuel GallegosNo ratings yet
- MCQ Final 2014Document19 pagesMCQ Final 2014JohnSon100% (1)
- Serious Adverse Events of Special Interest Following mRNA COVID-19 Vaccination in Randomized Trials in AdultsDocument9 pagesSerious Adverse Events of Special Interest Following mRNA COVID-19 Vaccination in Randomized Trials in AdultsLilianneNo ratings yet
- Case Study 7 - Antepartum BleedingDocument2 pagesCase Study 7 - Antepartum BleedingRahul Tharwani100% (1)
- 445 1045 1 PBDocument6 pages445 1045 1 PBAnnisa Dhiya UlhaqNo ratings yet
- Errors 2Document5 pagesErrors 2Anggun rahmi PutriNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Assessment of Hematologic Disorders - Physical AssessmentDocument3 pagesAssessment of Hematologic Disorders - Physical AssessmentUSC Upstate Nursing CoachesNo ratings yet
- The Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesDocument9 pagesThe Importance of Proteinuria in Preeclampsia and Its Predictive Role in Maternal and Neonatal OutcomesimuhammadfahmiNo ratings yet
- Perfusion Concept MapDocument1 pagePerfusion Concept Mapapi-639782898No ratings yet