You might also like
- Endocrine, USMLE ENDPOINTDocument73 pagesEndocrine, USMLE ENDPOINTDaNy Chiriac50% (2)
- Family Jewels - Hardy HabermanDocument55 pagesFamily Jewels - Hardy HabermanRoland TamásNo ratings yet
- Anatomy - Pectoral Region and Axilla PDFDocument4 pagesAnatomy - Pectoral Region and Axilla PDFAngel KimNo ratings yet
- Freemasonry Uncovering FreemasonryDocument113 pagesFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- Medad Andrology Special Note NMT13 PDFDocument70 pagesMedad Andrology Special Note NMT13 PDFSelim TarekNo ratings yet
- WEEK 1 - Chapter 16 - Lymphatic System and ImmunityDocument59 pagesWEEK 1 - Chapter 16 - Lymphatic System and ImmunityOliver Namyalo100% (1)
- Final Case Study (Hernia)Document52 pagesFinal Case Study (Hernia)Kingfer Garcia Ignacio II63% (16)
- Softcopy For Teachers PDFDocument199 pagesSoftcopy For Teachers PDFMithalina AfiqahNo ratings yet
- Revision of The Venous System - The Role of The Vertebral VeinsDocument12 pagesRevision of The Venous System - The Role of The Vertebral Veinsgiomic1973No ratings yet
- Fnhum 09 00407Document8 pagesFnhum 09 00407Nakarit SangsirinawinNo ratings yet
- 2802 FullDocument9 pages2802 FullNatalia NuñezNo ratings yet
- Basic TmsDocument7 pagesBasic TmsNakarit SangsirinawinNo ratings yet
- 1 s2.0 S1388245719310041 MainDocument1 page1 s2.0 S1388245719310041 MainMohamed AbdoNo ratings yet
- Fnmol 13 528396Document12 pagesFnmol 13 528396Nakarit SangsirinawinNo ratings yet
- Transcallosally Mediated InhibitionDocument11 pagesTranscallosally Mediated InhibitiongiacomopinaliNo ratings yet
- Journal Pone 0035080Document12 pagesJournal Pone 0035080Juan Carlos Guerrero RNo ratings yet
- Jneurosci 5316-03 2004Document7 pagesJneurosci 5316-03 2004labsoneducationNo ratings yet
- Quartarone 2004Document11 pagesQuartarone 2004vanogig777No ratings yet
- Abstracts / Brain Stimulation 10 (2017) 346 E540 396Document1 pageAbstracts / Brain Stimulation 10 (2017) 346 E540 396Aleja ToPaNo ratings yet
- Nitsche 2004Document5 pagesNitsche 2004Larissa OliveiraNo ratings yet
- Journal Pone 0030971Document10 pagesJournal Pone 0030971hsiangaldazosaNo ratings yet
- Akinesia in Parkinsons Disease 1 Shortening of Simple Reaction Time W Focal Single Pulse TMSDocument10 pagesAkinesia in Parkinsons Disease 1 Shortening of Simple Reaction Time W Focal Single Pulse TMSadit020586No ratings yet
- #6479 Bliem B 2008Document12 pages#6479 Bliem B 2008marcu_ruxandraNo ratings yet
- Repetitive Transcranial Magnetic Stimulation and TDCS in Motor Rehab After StrokeDocument5 pagesRepetitive Transcranial Magnetic Stimulation and TDCS in Motor Rehab After StrokelabsoneducationNo ratings yet
- Motor Cortex Disinhibition in Alzheimer'S Disease: J. Liepert, K.J. Baèr, U. Meske, C. WeillerDocument6 pagesMotor Cortex Disinhibition in Alzheimer'S Disease: J. Liepert, K.J. Baèr, U. Meske, C. WeillerDiego Saavedra LizanaNo ratings yet
- TMP E946Document7 pagesTMP E946FrontiersNo ratings yet
- ScienceDocument6 pagesScienceJulian SotoNo ratings yet
- NIH Public Access: Transcranial Magnetic Stimulation and Aphasia RehabilitationDocument19 pagesNIH Public Access: Transcranial Magnetic Stimulation and Aphasia RehabilitationadiNo ratings yet
- Transcranial MagneticDocument19 pagesTranscranial Magneticyaang yuliana ciptaNo ratings yet
- Basic Ppes of TMEDocument6 pagesBasic Ppes of TMELorena PérezNo ratings yet
- JMD 19083Document3 pagesJMD 19083anton MDNo ratings yet
- Electrical Stimulation Over Muscle Tendons in HumansDocument8 pagesElectrical Stimulation Over Muscle Tendons in Humansaselaar5536No ratings yet
- Rogasch Et Al. 2013Document9 pagesRogasch Et Al. 2013yossi.zanaNo ratings yet
- Enhancement of Cortical Excitanbility and LL Motor Function in Troke Patient by TDCSDocument6 pagesEnhancement of Cortical Excitanbility and LL Motor Function in Troke Patient by TDCSlabsoneducationNo ratings yet
- Magnetoelectric Brain Stimulation in TheDocument9 pagesMagnetoelectric Brain Stimulation in ThesukohomaNo ratings yet
- PDFDocument8 pagesPDFshalvinNo ratings yet
- Distilling The Source of Transcranial Evoked PotentialsDocument3 pagesDistilling The Source of Transcranial Evoked PotentialsRaaj ChatterjeeNo ratings yet
- Excitability Modulation of The Motor Sys PDFDocument12 pagesExcitability Modulation of The Motor Sys PDFСтанислав ЗубковNo ratings yet
- 2.3 Current Source For Current Density Imaging in Multi-Electrode NeurostimulationDocument4 pages2.3 Current Source For Current Density Imaging in Multi-Electrode Neurostimulationabrar al mahmoodNo ratings yet
- Applications of Transcranial Magnetic Stimulation TMS in Child and Adolescent PsychiatryDocument10 pagesApplications of Transcranial Magnetic Stimulation TMS in Child and Adolescent Psychiatryssky worthNo ratings yet
- Therapeutic Trial of Repetitive Transcranial Magnetic Stimulation After Acute Ischemic StrokeDocument3 pagesTherapeutic Trial of Repetitive Transcranial Magnetic Stimulation After Acute Ischemic StrokeAlex GasnasNo ratings yet
- CRPS Nardone - Et - Al-2018-Acta - Neurologica - ScandinavicaDocument7 pagesCRPS Nardone - Et - Al-2018-Acta - Neurologica - ScandinavicaJorge Dávila GonzálezNo ratings yet
- BHX 055Document13 pagesBHX 055Alfeku CabraNo ratings yet
- NITSCHE &PAULUS Excitability Changes Induced in The Human Motor Cortex by Weak Transcranial Direct Current StimulationDocument7 pagesNITSCHE &PAULUS Excitability Changes Induced in The Human Motor Cortex by Weak Transcranial Direct Current Stimulationexcelencia5No ratings yet
- Transcranial Electrical Stimulation (tES - TDCS TRNS, tACS) MethodsDocument17 pagesTranscranial Electrical Stimulation (tES - TDCS TRNS, tACS) MethodsGilson Mariano NeryNo ratings yet
- Monte Silva2010Document6 pagesMonte Silva2010GUSTAVO CARIBÉNo ratings yet
- Efeito Da Estimulação Magnética Transcraniana Repetitiva em Pacientes Com Disartria Após Acidente Vascular Cerebral SubagudoDocument7 pagesEfeito Da Estimulação Magnética Transcraniana Repetitiva em Pacientes Com Disartria Após Acidente Vascular Cerebral Subagudonathalia suellenNo ratings yet
- Fnbeh 12 00197Document13 pagesFnbeh 12 00197Carlos ANo ratings yet
- Transcranial Magnetic StimulationDocument2 pagesTranscranial Magnetic StimulationCandle Shop FullNo ratings yet
- Mammograms Lead To Invalid DiagnosesDocument6 pagesMammograms Lead To Invalid DiagnosesTeresa BeckNo ratings yet
- TDCS in Pediatric HemiparesisDocument1 pageTDCS in Pediatric HemiparesislabsoneducationNo ratings yet
- Schulz Gerloff Hummel 2013 Non Invasive Brain Stimulation in Neurological DiseasesDocument9 pagesSchulz Gerloff Hummel 2013 Non Invasive Brain Stimulation in Neurological DiseasesandreapalmapNo ratings yet
- Angius SRDocument23 pagesAngius SRShyamali Kaushalya FernandoNo ratings yet
- Bear&KirkwoodDocument11 pagesBear&KirkwoodswagatarcNo ratings yet
- Kerrigan 2004Document9 pagesKerrigan 2004Estereotaxia BrasilNo ratings yet
- Magnet 1Document14 pagesMagnet 1ahippoNo ratings yet
- Research 2Document2 pagesResearch 2builenhatminh02No ratings yet
- Article Review Samantha HaworthDocument4 pagesArticle Review Samantha HaworthSamantha HaworthNo ratings yet
- 1 s2.0 S2665945X22000067 MainDocument22 pages1 s2.0 S2665945X22000067 MainThonny EspinosaNo ratings yet
- EJHM - Volume 84 - Issue 1 - Pages 1801-1809-2Document9 pagesEJHM - Volume 84 - Issue 1 - Pages 1801-1809-2Diego Eduardo HurtadoNo ratings yet
- Spampinato Celnik 20Document10 pagesSpampinato Celnik 20vikhen0712No ratings yet
- Ijbms 19 800Document4 pagesIjbms 19 800wineniNo ratings yet
- 2016 - Horvath - Reaction-Time-tDCS Nosignificant Effectoftranscranialdirectcurrentstimulation (TDCS)Document9 pages2016 - Horvath - Reaction-Time-tDCS Nosignificant Effectoftranscranialdirectcurrentstimulation (TDCS)Shyamali Kaushalya FernandoNo ratings yet
- ArticleDocument11 pagesArticleSai RamNo ratings yet
- 2020 Non-Invasive Cerebellar Stimulation inDocument15 pages2020 Non-Invasive Cerebellar Stimulation inJefe de Escuela PsicologiaNo ratings yet
- 5990 FullDocument10 pages5990 FullRomina MendezBrandanNo ratings yet
- Techniques in Cognitive Neuroscience: Transcranial Magnetic Stimulation (TMS)Document33 pagesTechniques in Cognitive Neuroscience: Transcranial Magnetic Stimulation (TMS)girithik14No ratings yet
- 2003 Changes in Median Nerve Somatosensory Transmission and Motor OutputDocument12 pages2003 Changes in Median Nerve Somatosensory Transmission and Motor OutputchooNo ratings yet
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Document76 pagesSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasNo ratings yet
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDocument9 pagesOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNo ratings yet
- Neuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcDocument7 pagesNeuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcAlex GasnasNo ratings yet
- Hypoglosal Nerve PalsyDocument4 pagesHypoglosal Nerve PalsyAlex GasnasNo ratings yet
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaDocument6 pagesFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasNo ratings yet
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorDocument25 pagesMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasNo ratings yet
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceDocument4 pages"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasNo ratings yet
- Funke Et Al-2011-The Journal of PhysiologyDocument13 pagesFunke Et Al-2011-The Journal of PhysiologyAlex GasnasNo ratings yet
- Death PathologyDocument80 pagesDeath PathologyAlex GasnasNo ratings yet
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraDocument7 pagesPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasNo ratings yet
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument70 pagesCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasNo ratings yet
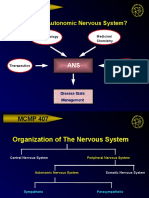
- MCMP 407: Why Study The Autonomic Nervous System?Document15 pagesMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasNo ratings yet
- LP9th - Cardiovascular SystemDocument5 pagesLP9th - Cardiovascular SystemOliver VillanuevaNo ratings yet
- Stretching: Mechanisms and Benefits For Sport Performance and Injury PreventionDocument19 pagesStretching: Mechanisms and Benefits For Sport Performance and Injury PreventionGeorge M. PamborisNo ratings yet
- Hipothalamus & HipofisisDocument42 pagesHipothalamus & HipofisisONe's IwanNo ratings yet
- Updated List of Dental Clinics As of September 2021Document4 pagesUpdated List of Dental Clinics As of September 2021Paolo Joshua Abratique0% (1)
- 4th Quarter Module 1Document6 pages4th Quarter Module 1Azziely-Arah Santiago PabroNo ratings yet
- Ocular SurfaceDocument81 pagesOcular Surfacechavali deepthiNo ratings yet
- 00004Document8 pages00004api-3710948No ratings yet
- (03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedDocument3 pages(03241750 - Acta Medica Bulgarica) Horseshoe Kidney With Hydronephrosis - Tales of The UnexpectedTeodorNo ratings yet
- Special Senses Part 1 (Taste & Smell)Document18 pagesSpecial Senses Part 1 (Taste & Smell)rizwanbas100% (1)
- Anatomy LE5 Samplex 2017BDocument6 pagesAnatomy LE5 Samplex 2017BHanako Sasaki AranillaNo ratings yet
- Homeostasis FSC Biology Notes Part 2 Chapter 15Document18 pagesHomeostasis FSC Biology Notes Part 2 Chapter 15yaseen shahNo ratings yet
- Chugh2010 Brodie PDFDocument7 pagesChugh2010 Brodie PDFLudy Jiménez ValdiviaNo ratings yet
- Z021 PDFDocument2 pagesZ021 PDFAditya RudraNo ratings yet
- Physiology Cardiovascular EquationsDocument2 pagesPhysiology Cardiovascular Equationsskim93No ratings yet
- Https://d1c0fc7ib89kee - Cloudfront.net/uploads/attachment/file//reproduction Exam QuestionDocument8 pagesHttps://d1c0fc7ib89kee - Cloudfront.net/uploads/attachment/file//reproduction Exam QuestionAmaya AliNo ratings yet
- Chapter 7 RH TypingDocument22 pagesChapter 7 RH TypingYo Issei Hyodono100% (1)
- ScienceGeography3ResourceSample PDFDocument9 pagesScienceGeography3ResourceSample PDFmargantoniNo ratings yet
- What Is Reproduction?: Male Reproductive System GenesDocument4 pagesWhat Is Reproduction?: Male Reproductive System GenesPrada Maya AnggariNo ratings yet
- Section - 026 - Immediate DenturesDocument12 pagesSection - 026 - Immediate DenturesMuli Maroshi100% (1)
- Kidney AnatomyDocument55 pagesKidney AnatomyMohammad zreadNo ratings yet
- Case Scenario 3 - Musco-Skeletal SystemDocument3 pagesCase Scenario 3 - Musco-Skeletal SystemWill KnightNo ratings yet
- 10 Palpasi Abdomen Dan Bagian Tubuh LainnyaDocument26 pages10 Palpasi Abdomen Dan Bagian Tubuh LainnyaSANGGA BUWANANo ratings yet