You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- S0003999321002963Document10 pagesS0003999321002963Nura Eky VNo ratings yet
- Orthography Development: Frank SeifartDocument26 pagesOrthography Development: Frank SeifartAnwar WafiNo ratings yet
- ISMST GuidelinesDocument112 pagesISMST GuidelinesDhrubo TaraNo ratings yet
- Overview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionDocument4 pagesOverview of Cardiac Valvular Disorders - Cardiovascular Disorders - MSD Manual Professional EditionNura Eky VNo ratings yet
- 3 Mode Exc OADocument7 pages3 Mode Exc OANura Eky VNo ratings yet
- Bloom's Taxonomy - WikipediaDocument11 pagesBloom's Taxonomy - WikipediaNura Eky VNo ratings yet
- PRM 5 20200018Document9 pagesPRM 5 20200018Nura Eky VNo ratings yet
- 1 s2.0 S0531556520305611 MainDocument8 pages1 s2.0 S0531556520305611 MainNura Eky VNo ratings yet
- OTAGO On FrailtyDocument5 pagesOTAGO On FrailtyNura Eky VNo ratings yet
- 1 s2.0 S1877065719301794 MainDocument8 pages1 s2.0 S1877065719301794 MainNura Eky VNo ratings yet
- Effect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialDocument10 pagesEffect of Different Types of Exercises On Psychological and Cognitive Features in People With Parkinson's Disease: A Randomized Controlled TrialNura Eky VNo ratings yet
- Impact of Covid Patient RecoveryDocument15 pagesImpact of Covid Patient RecoveryNura Eky VNo ratings yet
- ESWT in Chronic LBPDocument6 pagesESWT in Chronic LBPNura Eky VNo ratings yet
- 1 s2.0 S0003999321001404Document10 pages1 s2.0 S0003999321001404Nura Eky VNo ratings yet
- Pai Patton97PostPrintDocument7 pagesPai Patton97PostPrintNura Eky VNo ratings yet
- Relationship Between Frontal Knee Position and TheDocument12 pagesRelationship Between Frontal Knee Position and TheNura Eky VNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Polifarmasi and Fall in ElderlyDocument5 pagesPolifarmasi and Fall in ElderlyNura Eky VNo ratings yet
- Design CPMDocument5 pagesDesign CPMNura Eky VNo ratings yet
- Hof Condition For Dynamic StabilityDocument8 pagesHof Condition For Dynamic StabilityNura Eky VNo ratings yet
- Short Physical Performance Battery Protocol and Score Sheet: 1. Balance TestsDocument8 pagesShort Physical Performance Battery Protocol and Score Sheet: 1. Balance Testsruth lopezNo ratings yet
- Cryptogenic Stroke After Percutaneous Closure of ADocument6 pagesCryptogenic Stroke After Percutaneous Closure of ANura Eky VNo ratings yet
- Methods For Assessing Leg Length DiscrepancyDocument13 pagesMethods For Assessing Leg Length DiscrepancyKanika SinhaNo ratings yet
- Anterior Cruciate Ligament Injury-Who Succeeds WitDocument9 pagesAnterior Cruciate Ligament Injury-Who Succeeds WitNura Eky VNo ratings yet
- CASP RCT Checklist PDF Fillable FormDocument4 pagesCASP RCT Checklist PDF Fillable FormNura Eky VNo ratings yet
- Leonard, 2002Document18 pagesLeonard, 2002Nura Eky VNo ratings yet
- Obesity Review MelaninDocument12 pagesObesity Review MelaninNura Eky VNo ratings yet
- Keseimbangan Asam BasaDocument2 pagesKeseimbangan Asam BasaNura Eky VNo ratings yet
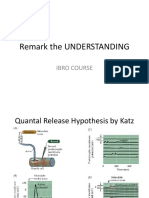
- Remark The UNDERSTANDING: Ibro CourseDocument4 pagesRemark The UNDERSTANDING: Ibro CourseNura Eky VNo ratings yet
- Spleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodDocument13 pagesSpleen: - Site of Lymphocyte Proliferation - Immune Surveillance and Response - Cleanses The BloodNura Eky VNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Advia Centaur SafetyDocument5 pagesAdvia Centaur SafetyMaduraiveeran cNo ratings yet
- Cardiac Cycle: DR Rakesh JainDocument97 pagesCardiac Cycle: DR Rakesh JainKemoy FrancisNo ratings yet
- Abreviaciones ChatDocument4 pagesAbreviaciones ChatrojarodNo ratings yet
- Ent AssessmentDocument23 pagesEnt AssessmentPdianghunNo ratings yet
- Difficult Airway AlgorithmDocument48 pagesDifficult Airway AlgorithmshikhaNo ratings yet
- Employers Guide - InteractiveDocument24 pagesEmployers Guide - Interactiveapi-285398586No ratings yet
- Patients' Perceptions of Barriers To Self-Managing Bipolar DisorderDocument10 pagesPatients' Perceptions of Barriers To Self-Managing Bipolar DisorderMilton MurilloNo ratings yet
- Case Studies - EditedDocument5 pagesCase Studies - EditedFunny LifeNo ratings yet
- Impact of Covid-19 in Our SocietyDocument25 pagesImpact of Covid-19 in Our SocietyAISHA 20682No ratings yet
- Food Industry TrainingDocument18 pagesFood Industry TrainingSumit KumarNo ratings yet
- Adoption Foster ApplicationDocument4 pagesAdoption Foster Applicationlb8757No ratings yet
- Pathophysiology of Typhoid FeverDocument3 pagesPathophysiology of Typhoid FeverKristofer Karlo Cabrera Castillo0% (1)
- Winter 2010 Natural FarmerDocument48 pagesWinter 2010 Natural FarmerV1xWqNo ratings yet
- Questions and Answers 1Document7 pagesQuestions and Answers 1api-382372564No ratings yet
- Regulation of Iron MetabolismDocument21 pagesRegulation of Iron MetabolismElita Maritan SNo ratings yet
- Belgian MalinoisDocument9 pagesBelgian MalinoislordnrNo ratings yet
- Kendriya Vidyalaya Kirandul: Investigatory Project of BiologyDocument10 pagesKendriya Vidyalaya Kirandul: Investigatory Project of BiologyAachal GayreNo ratings yet
- Perkutan Kateter Vena Sentral Dibandingkan Perifer Kanula Untuk Pengiriman Nutrisi Parenteral Ada NeonatusDocument3 pagesPerkutan Kateter Vena Sentral Dibandingkan Perifer Kanula Untuk Pengiriman Nutrisi Parenteral Ada NeonatusmuslihudinNo ratings yet
- Eye LubricantDocument9 pagesEye LubricantbuddhahandNo ratings yet
- Full Download Test Bank For Essentials of Genetics 8th Edition by Klug PDF Full ChapterDocument36 pagesFull Download Test Bank For Essentials of Genetics 8th Edition by Klug PDF Full Chapterfencingvesper9dgb04100% (17)
- Transforming Growth Factor Beta TGFBDocument8 pagesTransforming Growth Factor Beta TGFBxxxxxxxNo ratings yet
- Unit 4 ReadingDocument4 pagesUnit 4 ReadingElvantNo ratings yet
- Dr. Huang's 10 Relieving ProtocolsDocument5 pagesDr. Huang's 10 Relieving ProtocolsCarissa Nichols86% (7)
- Assessing The Ear and HearingDocument32 pagesAssessing The Ear and HearingArlyn Mendenilla0% (1)
- P.E 3A Learning Activity Sheet WEEK 5 6Document7 pagesP.E 3A Learning Activity Sheet WEEK 5 6Ris CorreaNo ratings yet
- Low-Dose Naltrexone (LDN) Fact Sheet 2016: Contact: Linda Elsegood Email: Skype Phone No'sDocument8 pagesLow-Dose Naltrexone (LDN) Fact Sheet 2016: Contact: Linda Elsegood Email: Skype Phone No'scristiNo ratings yet
- Glucagon and Its Metabolic EffectsDocument31 pagesGlucagon and Its Metabolic EffectsnikenNo ratings yet
- A Drug Study On PrednisoneDocument5 pagesA Drug Study On PrednisonePrincess Alane MorenoNo ratings yet
- Anatomy and Physiology of Male Reproductive SystemDocument8 pagesAnatomy and Physiology of Male Reproductive SystemAdor AbuanNo ratings yet
- Black SeedDocument26 pagesBlack SeedAslam Aly Saib100% (1)