You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Veterinary Clinical Pathology Lecture NotesDocument17 pagesVeterinary Clinical Pathology Lecture NotesShirley Faye Sales80% (5)
- D-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home CollectionDocument4 pagesD-37/1, TTC MIDC, Turbhe, Navi Mumbai-400 703: Name Ref. by Test Asked::: Patientid: Home Collectionfaiyaz432No ratings yet
- Blood Questions Human Physiology PDFDocument5 pagesBlood Questions Human Physiology PDFARUSHI ARVIND100% (2)
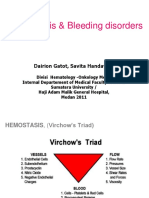
- HemostasisDocument48 pagesHemostasisBintang Ruth Cecilia FebrinaNo ratings yet
- CBC ReportsDocument2 pagesCBC ReportsIbrar Hussain100% (1)
- Blood Transfusion Service (2006)Document323 pagesBlood Transfusion Service (2006)Devie MaraNo ratings yet
- Ipi 431590Document8 pagesIpi 431590Pekemon Shufle AsiaNo ratings yet
- ItpDocument3 pagesItpPekemon Shufle AsiaNo ratings yet
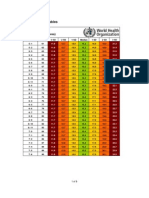
- Z Score Girls BMIDocument6 pagesZ Score Girls BMIVienny Widhyanti Rosarya100% (1)
- 033 26781am100914 253 257Document5 pages033 26781am100914 253 257Pekemon Shufle AsiaNo ratings yet
- 7.abstrak ENGDocument1 page7.abstrak ENGPekemon Shufle AsiaNo ratings yet
- Qwkdjasdja LSD Laskf 'Aslf A SF As Fas F Asf As F SF As Fa SF As Fas F Saf As F Asf Sa Fa Sfasfas Fa SCXZVXZCB CVN GH KDocument2 pagesQwkdjasdja LSD Laskf 'Aslf A SF As Fas F Asf As F SF As Fa SF As Fas F Saf As F Asf Sa Fa Sfasfas Fa SCXZVXZCB CVN GH KPekemon Shufle AsiaNo ratings yet
- Yoptumyfkpp GDL Sistimeiry 72 1 SistiDocument13 pagesYoptumyfkpp GDL Sistimeiry 72 1 SistiPekemon Shufle AsiaNo ratings yet
- Frequencies: FREQUENCIES VARIABLES Klasifikasi /order AnalysisDocument6 pagesFrequencies: FREQUENCIES VARIABLES Klasifikasi /order AnalysisPekemon Shufle AsiaNo ratings yet
- 7.abstrak ENGDocument1 page7.abstrak ENGPekemon Shufle AsiaNo ratings yet
- Inter RaterDocument3 pagesInter RaterBambang AdiNo ratings yet
- Eticket TDHXYYDocument2 pagesEticket TDHXYYTirta BudiawanNo ratings yet
- DD Nyeri Perut Kanan BawahDocument3 pagesDD Nyeri Perut Kanan BawahPekemon Shufle AsiaNo ratings yet
- SpondylolisthesisDocument8 pagesSpondylolisthesisPekemon Shufle AsiaNo ratings yet
- LampiranDocument9 pagesLampiranPekemon Shufle AsiaNo ratings yet
- The Limping ChildDocument4 pagesThe Limping ChildPekemon Shufle AsiaNo ratings yet
- LampiranDocument9 pagesLampiranPekemon Shufle AsiaNo ratings yet
- Intro. To Medtech AssignmentDocument8 pagesIntro. To Medtech AssignmentStephanie OlleroNo ratings yet
- Biology Project: C XIBDocument18 pagesBiology Project: C XIBPranjal SharmaNo ratings yet
- HemoglobinDocument15 pagesHemoglobinArya RaoNo ratings yet
- DOH NVBSP OverviewDocument32 pagesDOH NVBSP OverviewAmor Taripe100% (1)
- Understanding Transfusion Reactions in Oncology by NurseDocument6 pagesUnderstanding Transfusion Reactions in Oncology by NursefitriNo ratings yet
- BMLT Class Note On Anemia ClassificationDocument2 pagesBMLT Class Note On Anemia ClassificationSubhasish BarikNo ratings yet
- Reading Skill PBTDocument20 pagesReading Skill PBTGesa HayuNo ratings yet
- 273 615 1 PBDocument6 pages273 615 1 PBIkki MarphyNo ratings yet
- Immune Thrombocytopenia in The Newborn: Murat YurdakökDocument10 pagesImmune Thrombocytopenia in The Newborn: Murat YurdakökEunice RiveraNo ratings yet
- Blood Group Testing: Hong-Yang Li and Kai GuoDocument11 pagesBlood Group Testing: Hong-Yang Li and Kai Guodkp rbmNo ratings yet
- Cancer-And Chemotherapy - Induced Anemia: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document54 pagesCancer-And Chemotherapy - Induced Anemia: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Hataitap ChonchepNo ratings yet
- Chapter 42Document3 pagesChapter 42Soc Gerren TuasonNo ratings yet
- AFP/PNP Housing, San Isidro, Rodriguez, RizalDocument1 pageAFP/PNP Housing, San Isidro, Rodriguez, RizalChristine ApoloNo ratings yet
- MY Hematology MasterclassDocument32 pagesMY Hematology Masterclassabdul qayyumNo ratings yet
- Rabbithematology PDFDocument12 pagesRabbithematology PDFHuda HudaNo ratings yet
- Hemostasis Basics Programmed Learner: TopicDocument19 pagesHemostasis Basics Programmed Learner: TopicAahsan Iqbal احسن اقبالNo ratings yet
- PancitopeniasDocument34 pagesPancitopeniasJuan Pablo Fuentes ArriagadaNo ratings yet
- MD 13004Document5 pagesMD 13004SirNo ratings yet
- Other Blood Groups: Mnss Blood Group SystemDocument7 pagesOther Blood Groups: Mnss Blood Group SystemDaena TimtimanNo ratings yet
- Transfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDocument3 pagesTransfusion - March April 1966 - Allen - Choice of Blood For Exchange TransfusionDR. KHANNo ratings yet
- Signs of VTE Infographic PDFDocument1 pageSigns of VTE Infographic PDFJulia Martha LinardiNo ratings yet
- Hematology 2023Document775 pagesHematology 2023Internsip RS SK Lerik100% (1)
- Course Code: NSC 410 Course Title: Practicum and Teaching Methodology MATRIC NUMBER: 19001748Document6 pagesCourse Code: NSC 410 Course Title: Practicum and Teaching Methodology MATRIC NUMBER: 19001748Kenan Gawinan KekeNo ratings yet
- In2Med HaematologyDocument30 pagesIn2Med Haematologye148659No ratings yet