You might also like
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- CPC Exam Review QuestionsDocument3 pagesCPC Exam Review QuestionshevinpatelNo ratings yet
- Clinical Cases For MRCPCH PART 2 Applied Knowledge in PracticeDocument218 pagesClinical Cases For MRCPCH PART 2 Applied Knowledge in Practiceaeyousef88% (16)
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- Understanding-Ocd 2016 v2Document27 pagesUnderstanding-Ocd 2016 v2Samanjit Sen Gupta100% (1)
- Nutrition in PregnancyDocument48 pagesNutrition in PregnancyGladstone AsadNo ratings yet
- Neonatal Emergencies FinalDocument90 pagesNeonatal Emergencies FinalDr Raseena VattamkandathilNo ratings yet
- Alzheimer's DiseaseDocument469 pagesAlzheimer's DiseaseGastón G. Fernández100% (3)
- A Polymerase Chain Reaction-Based Algorithm To Detect and Prevent Transmission of Adenoviral Conjunctivitis in Hospital EmployeesDocument10 pagesA Polymerase Chain Reaction-Based Algorithm To Detect and Prevent Transmission of Adenoviral Conjunctivitis in Hospital EmployeesWiyaah AsNo ratings yet
- Bacterial KeratitisDocument6 pagesBacterial KeratitisMelia RahmayantiNo ratings yet
- Jurnal Mata 1Document9 pagesJurnal Mata 1marhayudi15No ratings yet
- Queratitis BacterianaDocument5 pagesQueratitis BacterianaRichi CiriacoNo ratings yet
- Hospital - Base Epidemiology, Risk Factors and Microbiological Diagnosis of Bacterial Corneal UlcerDocument5 pagesHospital - Base Epidemiology, Risk Factors and Microbiological Diagnosis of Bacterial Corneal UlcerSilih Pulihan MedrofaNo ratings yet
- Jurnal Lensa Kontak TerbaruDocument22 pagesJurnal Lensa Kontak TerbaruNiSa Ka Al-LuLuNo ratings yet
- Jurnal MataDocument28 pagesJurnal MatamarinatamiNo ratings yet
- Schechter 2015Document8 pagesSchechter 2015joseph rivaldoNo ratings yet
- Jurnal Nirza MataDocument15 pagesJurnal Nirza MataRozans IdharNo ratings yet
- Bak TeriDocument4 pagesBak TeriHawania IINo ratings yet
- CorinebakteriumDocument6 pagesCorinebakteriummillaNo ratings yet
- Microbiological Profile and Antimicrobial Sensitivity Pattern of Culture Positive Bacterial Keratitis: A Prospective Observational StudyDocument5 pagesMicrobiological Profile and Antimicrobial Sensitivity Pattern of Culture Positive Bacterial Keratitis: A Prospective Observational StudyBombong NurpaginoNo ratings yet
- A Study On Clinico-Etiological Profile of Mycotic Keratitis in Tertiary Care Hospital at Government Medical College, Kota (Rajasthan)Document7 pagesA Study On Clinico-Etiological Profile of Mycotic Keratitis in Tertiary Care Hospital at Government Medical College, Kota (Rajasthan)IJAR JOURNALNo ratings yet
- CDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexDocument16 pagesCDC Repeat Syphilis Infection and HIV Coinfection Among Men Who Have SexkikiNo ratings yet
- Review Article: Profile of Corneal Ulcer in A Tertiary Eye Care CentreDocument6 pagesReview Article: Profile of Corneal Ulcer in A Tertiary Eye Care CentreNadhila ByantNo ratings yet
- A Retrospective Study of Bacterial Keratitis in Bundelkhand RegionDocument4 pagesA Retrospective Study of Bacterial Keratitis in Bundelkhand RegionPangeran CintaNo ratings yet
- Moraxella Keratitis: Analysis of Risk Factors, Clinical Characteristics, Management, and Treatment OutcomesDocument6 pagesMoraxella Keratitis: Analysis of Risk Factors, Clinical Characteristics, Management, and Treatment OutcomesNadira putri ArlanbiNo ratings yet
- Jurnal AntibiotikDocument4 pagesJurnal AntibiotikYuli IndrawatiNo ratings yet
- Bacteriological Profile and Drug Susceptibility Patterns in Dacryocystitis Patients Attending Gondar University Teaching Hospital, Northwest EthiopiaDocument17 pagesBacteriological Profile and Drug Susceptibility Patterns in Dacryocystitis Patients Attending Gondar University Teaching Hospital, Northwest EthiopiaDaisa RosianaNo ratings yet
- 2016 Article 294 PDFDocument7 pages2016 Article 294 PDFChato Haviz DanayomiNo ratings yet
- A Clinicopathological Study of Vernal Conjunctivitis in Urban and Rural Areas of Eastern India: A Hospital Based StudyDocument8 pagesA Clinicopathological Study of Vernal Conjunctivitis in Urban and Rural Areas of Eastern India: A Hospital Based StudyMuhammad AbdillahNo ratings yet
- Jceh 12 30 021Document3 pagesJceh 12 30 021Tatik HandayaniNo ratings yet
- Fungal Keratitis in Developing CountriesDocument11 pagesFungal Keratitis in Developing CountriesChikita Rizqi HanifatiNo ratings yet
- Vancomycin-Resistant Gram-Positive Bacterial Endophthalmitis: Epidemiology, Treatment Options, and OutcomesDocument4 pagesVancomycin-Resistant Gram-Positive Bacterial Endophthalmitis: Epidemiology, Treatment Options, and OutcomesFitria FerraraNo ratings yet
- JurnalMata Pigrum Keratitis 1471-2415!13!31Document4 pagesJurnalMata Pigrum Keratitis 1471-2415!13!31Alfrino Patriando AdamNo ratings yet
- Acanthamoeba Keratitis (AK) Is An Infection Associated To Prolonged Usage of ContactDocument8 pagesAcanthamoeba Keratitis (AK) Is An Infection Associated To Prolonged Usage of ContactLeah CamangonNo ratings yet
- A Study of Types of Corneal Ulcer and Their Causes in The Patient Attend Ophthalmology Department SRMS ImsDocument19 pagesA Study of Types of Corneal Ulcer and Their Causes in The Patient Attend Ophthalmology Department SRMS ImsPANKAJ KUMARNo ratings yet
- Candidiasis in PICUDocument6 pagesCandidiasis in PICUMeirinda HidayantiNo ratings yet
- Keratoconus An Updated Review PDFDocument26 pagesKeratoconus An Updated Review PDFMaria Jose SanjinesNo ratings yet
- Journal of KeratitisDocument16 pagesJournal of KeratitisAan AchmadNo ratings yet
- Spectrum of Fungal Keratitis: Clinicopathologic Study of 44 CasesDocument4 pagesSpectrum of Fungal Keratitis: Clinicopathologic Study of 44 CasesRichardNo ratings yet
- Comparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisDocument6 pagesComparative Study On The Efficacy of Non-Steroidal, Steroid and Non-Use Anti Inflammatory in The Treatment of Epidemic ConjungtivitisVisakha VidyadeviNo ratings yet
- AgashemicrosporidiaDocument5 pagesAgashemicrosporidiargroup331No ratings yet
- Lacrimal Duct Occlusion Is Associated With Infectious KeratitisDocument6 pagesLacrimal Duct Occlusion Is Associated With Infectious KeratitisekaNo ratings yet
- Clinico-Microbiological Study of Pyodermas: Research Article Janardhan. B, Prasad - GK, Nandeshwar - AJ and Vidyavathi.NDocument5 pagesClinico-Microbiological Study of Pyodermas: Research Article Janardhan. B, Prasad - GK, Nandeshwar - AJ and Vidyavathi.NradiNo ratings yet
- Disease: Bacterial KeratitisDocument9 pagesDisease: Bacterial KeratitisDwi Ayu PrimadanaNo ratings yet
- Journal - Bilateral Simultaneous Infective KeratitisDocument4 pagesJournal - Bilateral Simultaneous Infective KeratitisAndayanaIdhamNo ratings yet
- Experimental Study On Cryotherapy For Fungal Corneal Ulcer: Researcharticle Open AccessDocument9 pagesExperimental Study On Cryotherapy For Fungal Corneal Ulcer: Researcharticle Open AccessSusPa NarahaNo ratings yet
- Prevalence and Prognosis of Corneal Perforation Patient in Beijing ChinaDocument4 pagesPrevalence and Prognosis of Corneal Perforation Patient in Beijing Chinaalifah syarafinaNo ratings yet
- Laboratory Diagnosis and Prevalence Study: of Corneal Infections From A Tertiary Eye Care HospitalDocument5 pagesLaboratory Diagnosis and Prevalence Study: of Corneal Infections From A Tertiary Eye Care HospitalSilih Pulihan MedrofaNo ratings yet
- DIAGNOSIS AND MANAGEMENT OF ENDOGENOUS ENDOPHTHALMITISDocument24 pagesDIAGNOSIS AND MANAGEMENT OF ENDOGENOUS ENDOPHTHALMITISBenk Setsuna F. SeieiNo ratings yet
- Crs LinDocument4 pagesCrs LinPoolerErNo ratings yet
- Jurnal Contact LensDocument0 pagesJurnal Contact LensDinka RoselyNo ratings yet
- Epidemiology of Bacterial Keratitis in A Referral Centre in South IndiaDocument7 pagesEpidemiology of Bacterial Keratitis in A Referral Centre in South IndiaHariharan VenkatasubramanianNo ratings yet
- Jurnal Conclusion - How Important Performing Direct Examination in Corneal Ulcer CasesDocument5 pagesJurnal Conclusion - How Important Performing Direct Examination in Corneal Ulcer CasessyramadhantiNo ratings yet
- PanaceaJMedSci 11 2 289 296Document8 pagesPanaceaJMedSci 11 2 289 296Jenerio PanggabeanNo ratings yet
- Clinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaDocument12 pagesClinical Spectrum and Antibiogram of Acinetobacter Infections in Children Study From A Tertiary Care Centre, IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- KeratitisDocument11 pagesKeratitisAnonymous mvNUtwidNo ratings yet
- Conjunctivitis As A Manifestation of Wegener 'S GranulomatosisDocument5 pagesConjunctivitis As A Manifestation of Wegener 'S GranulomatosisAsd DsaNo ratings yet
- (03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesDocument8 pages(03241750 - Acta Medica Bulgarica) Fungal Peritonitis Due To Gastroduodenal Perforation - Diagnostic and Treatment ChallengesTeodorNo ratings yet
- And Treatment Blepharokeratoconjunctivitis in Children: DiagnosisDocument5 pagesAnd Treatment Blepharokeratoconjunctivitis in Children: DiagnosislordaponkNo ratings yet
- Otomycosis in CSOM Patients Effectively Treated with Clotrimazole Ear DropsDocument4 pagesOtomycosis in CSOM Patients Effectively Treated with Clotrimazole Ear DropsShovie Thalia MirandaNo ratings yet
- Microbes Associated with Keratitis and Antibiotic SensitivityDocument6 pagesMicrobes Associated with Keratitis and Antibiotic SensitivityBima RizkiNo ratings yet
- Diagnosis and Management of Microbial Keratitis: AIOS Guidelines ForDocument24 pagesDiagnosis and Management of Microbial Keratitis: AIOS Guidelines ForKukuh Rizwido PrasetyoNo ratings yet
- Two Cases of An Atypical Presentation of Necrotizing StomatitisDocument5 pagesTwo Cases of An Atypical Presentation of Necrotizing StomatitisSamehada SamaNo ratings yet
- Piis0002939410000668 PDFDocument6 pagesPiis0002939410000668 PDFJennifer ChávezNo ratings yet
- Moshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KeDocument7 pagesMoshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KesyramadhantiNo ratings yet
- Ibrahim 2009Document7 pagesIbrahim 2009MARIO STEFFANO ARCE COAQUERANo ratings yet
- Posted at The Institutional Resources For Unique Collection and Academic Archives at Tokyo Dental College, Available From Http://ir - Tdc.ac - JPDocument20 pagesPosted at The Institutional Resources For Unique Collection and Academic Archives at Tokyo Dental College, Available From Http://ir - Tdc.ac - JPwhiezardNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- YapssDocument9 pagesYapsslathifa_nurNo ratings yet
- 1824 7288 39 18Document8 pages1824 7288 39 18Justy GuavaNo ratings yet
- Jurnal Mata 5Document11 pagesJurnal Mata 5lathifa_nurNo ratings yet
- Presentation 1Document2 pagesPresentation 1lathifa_nurNo ratings yet
- Stir SugarDocument5 pagesStir Sugarlathifa_nurNo ratings yet
- Ice CreamDocument7 pagesIce Creamlathifa_nurNo ratings yet
- Variasi Elektroensefalografik Selama End Pemeliharaan Dan Anestesi BedahDocument15 pagesVariasi Elektroensefalografik Selama End Pemeliharaan Dan Anestesi Bedahlathifa_nurNo ratings yet
- 1824 7288 39 18Document8 pages1824 7288 39 18Justy GuavaNo ratings yet
- h5n1 Oxford JournalDocument24 pagesh5n1 Oxford Journallathifa_nurNo ratings yet
- 183 Difficult Airway Management (Gabungan)Document135 pages183 Difficult Airway Management (Gabungan)lathifa_nurNo ratings yet
- Jurnal Mata 4Document6 pagesJurnal Mata 4lathifa_nurNo ratings yet
- Direct Electrical Current Is A New Therapeutic Option For VitiligoDocument4 pagesDirect Electrical Current Is A New Therapeutic Option For Vitiligolathifa_nurNo ratings yet
- Operasi Pada TikusDocument8 pagesOperasi Pada Tikuslathifa_nurNo ratings yet
- Direct Electrical Current Is A New Therapeutic Option For VitiligoDocument4 pagesDirect Electrical Current Is A New Therapeutic Option For Vitiligolathifa_nurNo ratings yet
- Obes Jurnal Gastology and Hepatology IssuesDocument8 pagesObes Jurnal Gastology and Hepatology Issueslathifa_nurNo ratings yet
- Tugas Translet DiareDocument8 pagesTugas Translet Diarelathifa_nurNo ratings yet
- Jurnal Mata 5Document11 pagesJurnal Mata 5lathifa_nurNo ratings yet
- Skripsi - Makanan Cepat Saji 3 B.ingDocument8 pagesSkripsi - Makanan Cepat Saji 3 B.inglathifa_nurNo ratings yet
- ThalasemiaDocument11 pagesThalasemiaTita Siti NurhalaNo ratings yet
- Bronchi o Lot IsDocument11 pagesBronchi o Lot Islathifa_nurNo ratings yet
- Skripsi - Fast Food Am. J. Epidemiol.-2009-Moore-29-36Document8 pagesSkripsi - Fast Food Am. J. Epidemiol.-2009-Moore-29-36lathifa_nurNo ratings yet
- 400 Seismic MethodsDocument10 pages400 Seismic Methodslathifa_nurNo ratings yet
- Thermo Regulation 2Document25 pagesThermo Regulation 2lathifa_nurNo ratings yet
- Obes Jurnal Gastology and Hepatology IssuesDocument8 pagesObes Jurnal Gastology and Hepatology Issueslathifa_nurNo ratings yet
- Fs GisDocument21 pagesFs Gislathifa_nurNo ratings yet
- Print LabDocument2 pagesPrint Lablathifa_nurNo ratings yet
- 42fundus AngiographyDocument28 pages42fundus AngiographyHitesh SharmaNo ratings yet
- Int Obs PDFDocument37 pagesInt Obs PDFsurgeon77No ratings yet
- Rheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009Document9 pagesRheumatic Fever For All For DR Wilfredo Stokes B. Guatemala Nov 2,009drwstokes100% (1)
- List of Empanelled Hospitals in CGHS NagpurDocument58 pagesList of Empanelled Hospitals in CGHS NagpurRajatNo ratings yet
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDocument4 pagesChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZNo ratings yet
- Significance of Facebow Transfer: January 2020Document6 pagesSignificance of Facebow Transfer: January 2020Mahmoud Ibrahem maanNo ratings yet
- Type2 Diabetes HandoutDocument1 pageType2 Diabetes Handouthendra_darmawan_4No ratings yet
- 13 - Adverse Drug Reactions CausesDocument4 pages13 - Adverse Drug Reactions CausesRojas Evert AlonsoNo ratings yet
- Hypertension in PregnancyDocument18 pagesHypertension in Pregnancyshubham kumarNo ratings yet
- Health Check Template FormDocument2 pagesHealth Check Template Form백만호No ratings yet
- Acute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsDocument2 pagesAcute Respiratory Distress Syndrome Nursing Management and Interventions - NurseslabsSachin SinghNo ratings yet
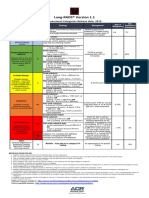
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Femoral Acetabular Impingement: RadiographyDocument9 pagesFemoral Acetabular Impingement: Radiography杨钦杰No ratings yet
- Artikel IlmiahDocument12 pagesArtikel IlmiahAsti NurchasanahNo ratings yet
- 5a.ESOPHAGEAL DISORDERSDocument16 pages5a.ESOPHAGEAL DISORDERSHayat AL AKOUMNo ratings yet
- Abu Dhabi DRGDocument62 pagesAbu Dhabi DRGDolly creationsNo ratings yet
- Effect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFDocument3 pagesEffect of Steam Inhalation On Nasal Mucociliary Clearance in Normal Individuals and Nasal Disease Sta PDFyolandaNo ratings yet
- Basic pharmacology of anaesthesia drugs in 40 charactersDocument56 pagesBasic pharmacology of anaesthesia drugs in 40 charactersrajvikram87No ratings yet
- Study On The Efficacy of Nosocomial Infection Control (Senic Project) - Summary of Study DesignDocument14 pagesStudy On The Efficacy of Nosocomial Infection Control (Senic Project) - Summary of Study DesignMunawir GazaliNo ratings yet
- Fetal risks of macrosomia in diabetic pregnanciesDocument27 pagesFetal risks of macrosomia in diabetic pregnanciesIful SaifullahNo ratings yet
- It 18 - Neonatal Seizure - HerDocument35 pagesIt 18 - Neonatal Seizure - HerRurie Awalia SuhardiNo ratings yet
- Delafloxacin 4Document23 pagesDelafloxacin 4Muhammad RamzanNo ratings yet