You might also like
- Reflux Laryngitis: An Update, 2009-2012: Philadelphia, Pennsylvania, and Ylancaster, CaliforniaDocument9 pagesReflux Laryngitis: An Update, 2009-2012: Philadelphia, Pennsylvania, and Ylancaster, CaliforniaJaime Crisosto AlarcónNo ratings yet
- Is Pepsin Detected in The Saliva of Patients Who Experience Pharyngeal Reflux?Document5 pagesIs Pepsin Detected in The Saliva of Patients Who Experience Pharyngeal Reflux?anon_740277752No ratings yet
- Sensitive Pepsin Immunoassay...Document6 pagesSensitive Pepsin Immunoassay...Peter SalimNo ratings yet
- Laryngopharyngeal Reflux Diagnosis, Treatment, and Latest ResearchDocument8 pagesLaryngopharyngeal Reflux Diagnosis, Treatment, and Latest ResearchfrizkapfNo ratings yet
- The Laryngoscope - 2019 - Weitzendorfer - Pepsin and Oropharyngeal PH Monitoring To Diagnose Patients WithDocument7 pagesThe Laryngoscope - 2019 - Weitzendorfer - Pepsin and Oropharyngeal PH Monitoring To Diagnose Patients WithfelitaNo ratings yet
- Saliva Pepsin Detection and Proton Pump Inhibitor Response in Suspected Laryngopharyngeal Re UxDocument6 pagesSaliva Pepsin Detection and Proton Pump Inhibitor Response in Suspected Laryngopharyngeal Re UxFuyumi RiaNo ratings yet
- 1678 4219 Ag s0004280320200000028 PDFDocument4 pages1678 4219 Ag s0004280320200000028 PDFTOMOKO TERUYANo ratings yet
- Upper GI Surgery for Laryngopharyngeal RefluxDocument4 pagesUpper GI Surgery for Laryngopharyngeal Refluxaulia sufarnapNo ratings yet
- Vaezi LPR More Questions Than Answers CC 2010Document8 pagesVaezi LPR More Questions Than Answers CC 2010Phoespha MayangSarieNo ratings yet
- Gerd in Subglottic StenosisDocument5 pagesGerd in Subglottic StenosisPantelis ChouridisNo ratings yet
- Wang 2012Document7 pagesWang 2012priskaNo ratings yet
- LPR vs GERD: Understanding the DifferenceDocument3 pagesLPR vs GERD: Understanding the DifferenceWilhelm HeinleinNo ratings yet
- PPI Role Laryngopharyngeal RefluxDocument5 pagesPPI Role Laryngopharyngeal RefluxROBINSON ELIOTT GONZ�LEZ P�EZNo ratings yet
- Aliment Pharmacol Ther - 2001 - Fackler - Ambulatory Gastric PH Monitoring Proper Probe Placement and Normal ValuesDocument8 pagesAliment Pharmacol Ther - 2001 - Fackler - Ambulatory Gastric PH Monitoring Proper Probe Placement and Normal ValuesSofia CorreaNo ratings yet
- Corpus GastritisDocument5 pagesCorpus Gastritisameer143No ratings yet
- Reflux LaryngitisDocument6 pagesReflux LaryngitisfahmimiraNo ratings yet
- PediatricsDocument7 pagesPediatricsbravoirvingNo ratings yet
- Lechien Saussez Karkos Curr Opin 2018Document12 pagesLechien Saussez Karkos Curr Opin 2018alivanabilafarinisaNo ratings yet
- Reflux and LaryngitisDocument7 pagesReflux and LaryngitisyannecaNo ratings yet
- 571 FullDocument7 pages571 FullMilav AliNo ratings yet
- Del Gaudio 2005Document12 pagesDel Gaudio 2005Rodrigo Felipe Toro MellaNo ratings yet
- Veterinary Internal Medicne - 2022 - Appelgrein - Quantification of Gastroesophageal Regurgitation in Brachycephalic DogsDocument8 pagesVeterinary Internal Medicne - 2022 - Appelgrein - Quantification of Gastroesophageal Regurgitation in Brachycephalic DogsRenato HortaNo ratings yet
- Monitoreo de Reflujo Ambulatorio para El Diagnóstico de La Enfermedad Por Reflujo Gastroesofágico Actualización Del Consenso de Oporto y Recomendaciones de Un Grupo de Consenso InternacionalDocument15 pagesMonitoreo de Reflujo Ambulatorio para El Diagnóstico de La Enfermedad Por Reflujo Gastroesofágico Actualización Del Consenso de Oporto y Recomendaciones de Un Grupo de Consenso Internacionalcaresq1340No ratings yet
- 1 s2.0 S0196070920301198 MainDocument5 pages1 s2.0 S0196070920301198 MainMeutia LaksaniNo ratings yet
- Clinical Manifestations and Role of Proton Pump Inhibitors in The Management of Laryngopharyngeal RefluxDocument12 pagesClinical Manifestations and Role of Proton Pump Inhibitors in The Management of Laryngopharyngeal RefluxElisa Vina JayantiNo ratings yet
- Globus Pharyngeus: A Review of Etiology, Diagnostics, and TreatmentDocument10 pagesGlobus Pharyngeus: A Review of Etiology, Diagnostics, and TreatmentMiguel QNo ratings yet
- Novel scintigraphic study finds asymptomatic volunteers experience upright gastroesophageal refluxDocument7 pagesNovel scintigraphic study finds asymptomatic volunteers experience upright gastroesophageal refluxMarylin Acuña HernándezNo ratings yet
- Saliva Transit and GERDDocument6 pagesSaliva Transit and GERDjmccoyNo ratings yet
- PH SalivaDocument5 pagesPH SalivaBia KneippNo ratings yet
- Esophageal Baseline Impedance Levels Diagnose NERDDocument8 pagesEsophageal Baseline Impedance Levels Diagnose NERDFhienovdhieyHa ThreuvHyNo ratings yet
- Background: Reflux LaryngitisDocument5 pagesBackground: Reflux LaryngitisElisa Vina JayantiNo ratings yet
- 38.park2006 Diagnosis of Laryngopharyngeal Reflux AmongDocument5 pages38.park2006 Diagnosis of Laryngopharyngeal Reflux AmongWahyu JuliandaNo ratings yet
- 4) bilis y acidoDocument7 pages4) bilis y acidopbchantaNo ratings yet
- Changing Trends of Color of Different Laryngeal Regions in Laryngopharyngeal Reflux DiseaseDocument5 pagesChanging Trends of Color of Different Laryngeal Regions in Laryngopharyngeal Reflux DiseaseNoviTrianaNo ratings yet
- 17 Ambulatory-pH-and-Impedance-Monitoring CLC Mortensen 2019Document3 pages17 Ambulatory-pH-and-Impedance-Monitoring CLC Mortensen 2019Judy AncyNo ratings yet
- Aga: Clinical Practice UpdateDocument12 pagesAga: Clinical Practice UpdatextineNo ratings yet
- GERD SchwartzDocument10 pagesGERD SchwartzMina Tharwat AzerNo ratings yet
- Laryngopharyngeal Reflux and Atypical GERD 2019Document16 pagesLaryngopharyngeal Reflux and Atypical GERD 2019Thespian VentrueNo ratings yet
- Final-clean-Revised Version Respiratory Manifestations GERDocument11 pagesFinal-clean-Revised Version Respiratory Manifestations GERDewiNo ratings yet
- Clinical Medicine Insights: Ear, Nose, ThroatDocument5 pagesClinical Medicine Insights: Ear, Nose, ThroatagustinadianasariaguNo ratings yet
- Pendekatan Diagnostik Refluks Laring Faring: Karin I. Rompas, Steward K. Mengko, Ora Et Labora I. PalandengDocument9 pagesPendekatan Diagnostik Refluks Laring Faring: Karin I. Rompas, Steward K. Mengko, Ora Et Labora I. PalandengFannyNo ratings yet
- Stricture EsofagealDocument11 pagesStricture EsofagealInes Camilla PutriNo ratings yet
- Original Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialDocument9 pagesOriginal Articles: Proton Pump Inhibitor Therapy For Chronic Laryngo-Pharyngitis: A Randomized Placebo-Control TrialAnonymous iM2totBrNo ratings yet
- Laparoscopic and Open Nissen Fundoplication: Preoperative EvaluationDocument11 pagesLaparoscopic and Open Nissen Fundoplication: Preoperative EvaluationLuis FelipeNo ratings yet
- 55.wilson1989pharyngoesophageal DysmotilityDocument5 pages55.wilson1989pharyngoesophageal DysmotilityWahyu JuliandaNo ratings yet
- LkjkusteiDocument8 pagesLkjkusteiPeriyasami GovindasamyNo ratings yet
- LPRDocument6 pagesLPRGoranJankovicNo ratings yet
- Hubungan Nilai PH Cairan Pleura Dengan Hasil Pleur PDFDocument6 pagesHubungan Nilai PH Cairan Pleura Dengan Hasil Pleur PDFHerliNo ratings yet
- Alimentary Pharmacology & TherapeuticsDocument7 pagesAlimentary Pharmacology & TherapeuticsArchie TobiasNo ratings yet
- Laryngeal Manifestations of Gastroesophageal Reflux DiseaseDocument7 pagesLaryngeal Manifestations of Gastroesophageal Reflux DiseaseAna BrankovićNo ratings yet
- Effect of An Antireflux Bed Wedge On Gastro Esophageal Reflux Symptoms and Acid Reflux 1467Document5 pagesEffect of An Antireflux Bed Wedge On Gastro Esophageal Reflux Symptoms and Acid Reflux 1467abel assefaNo ratings yet
- Literatur - Rohs, Et - Al. Esomeprazole Compared To Other PPIsDocument9 pagesLiteratur - Rohs, Et - Al. Esomeprazole Compared To Other PPIsChristine LilyanaNo ratings yet
- Joevence - Journal ArticleDocument15 pagesJoevence - Journal ArticleJoevence CuaresmaNo ratings yet
- Role of Gastroesophageal Reflux Disease in Asthmatic PatientsDocument10 pagesRole of Gastroesophageal Reflux Disease in Asthmatic PatientsWindy Gigiers SeptianiNo ratings yet
- Anticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)Document5 pagesAnticholinergic Medication Use Is Associated With Globus Pharyngeus (HAFT 2016)DANDYNo ratings yet
- Laryng Reflux 090825Document12 pagesLaryng Reflux 090825Putri SilviaNo ratings yet
- Diagnosis and Management of Functional HeartburnDocument9 pagesDiagnosis and Management of Functional Heartburnal ghiffari muhammad rayhanNo ratings yet
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesFrom EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- MS Prelim Exam ReviewerDocument9 pagesMS Prelim Exam ReviewerSheril100% (2)
- Gastrointestinal Tract Disorders Upper Lower Organ: Stomatitis (Dietcd) Gastritis GerdDocument125 pagesGastrointestinal Tract Disorders Upper Lower Organ: Stomatitis (Dietcd) Gastritis GerdAnonymous rzPX6lUNo ratings yet
- Dyspepsia Hypertension 1Document32 pagesDyspepsia Hypertension 1Jeno Luis AcubNo ratings yet
- Is It Ethical to Brand This ConditionDocument4 pagesIs It Ethical to Brand This Conditionfabian dionNo ratings yet
- GERD and Hiatal Hernia GuideDocument4 pagesGERD and Hiatal Hernia GuideAmoroso, Marian Corneth D.No ratings yet
- Bmj-2021-069211.full Reduce Unnecessary Use of Proton Pump InhibitorsDocument7 pagesBmj-2021-069211.full Reduce Unnecessary Use of Proton Pump InhibitorsYo MeNo ratings yet
- DRUGSDocument5 pagesDRUGSDanica EspejoNo ratings yet
- 1 Week Gastritis Diet Plan (My Personal Experience)Document8 pages1 Week Gastritis Diet Plan (My Personal Experience)ps piasNo ratings yet
- 7 Low Acid FoodsDocument7 pages7 Low Acid FoodsIce BibovskiNo ratings yet
- Pediatrics 2010 Thakkar E925 30Document8 pagesPediatrics 2010 Thakkar E925 30ivanhariachandraNo ratings yet
- Barralvisceral Bi Study Guide SamplerDocument47 pagesBarralvisceral Bi Study Guide SamplerLuulaa Minguin Garcia100% (8)
- The Effect of Thickened-Feed Interventions On Gastroesophageal RefluxDocument13 pagesThe Effect of Thickened-Feed Interventions On Gastroesophageal Refluxminerva_stanciuNo ratings yet
- GIDocument47 pagesGIJuliaNo ratings yet
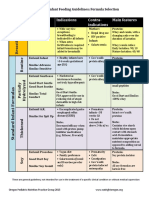
- Formula Selection OPNPGDocument2 pagesFormula Selection OPNPGRina PratiwiNo ratings yet
- Haad 3 Questions GiDocument16 pagesHaad 3 Questions GiPatpat De Guzman67% (3)
- HIATAL HERNIA PPT Final PDFDocument49 pagesHIATAL HERNIA PPT Final PDFregysujit60% (5)
- SMK 01Document12 pagesSMK 01FathiyaNo ratings yet
- Modified Inspiratory Muscle Training (m-IMT) As Promising Treatment For Gastro-Oesophageal Reflux Disease (GERD)Document5 pagesModified Inspiratory Muscle Training (m-IMT) As Promising Treatment For Gastro-Oesophageal Reflux Disease (GERD)B RGNo ratings yet
- Laryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNDocument4 pagesLaryngomalaci 2016 Ajoshua Bedwell, MD, GeorgeZalzal, MDNwawa chenNo ratings yet
- Test Bank For Medical Physiology 3rd Edition Walter Boron Emile BoulpaepDocument3 pagesTest Bank For Medical Physiology 3rd Edition Walter Boron Emile BoulpaepMisti Keane100% (25)
- Drug Study (MS)Document9 pagesDrug Study (MS)Kristine GallardoNo ratings yet
- Letters Combined (11 Referral, 2 Discharge, 1 Transfer)Document49 pagesLetters Combined (11 Referral, 2 Discharge, 1 Transfer)Faisal ImtiazNo ratings yet
- Candida EsofagitisDocument5 pagesCandida EsofagitisVina IsmawatiNo ratings yet
- Videofluoroscopic Swallowing StudiesDocument25 pagesVideofluoroscopic Swallowing StudiesPriisciilla Vicencio100% (1)
- Gastroesophageal Reflux in Children and AdolescentsDocument20 pagesGastroesophageal Reflux in Children and AdolescentsruthmindosiahaanNo ratings yet
- MS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DDocument8 pagesMS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DShawn TejanoNo ratings yet
- Surgical Patient Body Composition Changes and Post-Operative RecoveryDocument52 pagesSurgical Patient Body Composition Changes and Post-Operative RecoveryDr-Shadi Meteir100% (1)
- Nursing Plan of Care - FinalDocument3 pagesNursing Plan of Care - Finalapi-642989736No ratings yet
- Peptic UlcerDocument6 pagesPeptic UlcerNader Smadi100% (1)
- Pediatric Feeding DisorderDocument74 pagesPediatric Feeding Disorderkklaudia.pszichoNo ratings yet