You might also like
- How To Read A CTGDocument31 pagesHow To Read A CTGAbdullah As'ad100% (1)
- Cardiac ExaminationDocument23 pagesCardiac ExaminationAreza Eka PermanaNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Cardiovascular BigDocument37 pagesCardiovascular Bigfaiz nasirNo ratings yet
- Heart MurmursDocument48 pagesHeart MurmursAhmed T Al-MomtinNo ratings yet
- Medicine 1 Final Practical Exam ReviewerDocument10 pagesMedicine 1 Final Practical Exam ReviewerTP RMadNo ratings yet
- Pathophysiology of AgingDocument5 pagesPathophysiology of AgingRemelou Garchitorena AlfelorNo ratings yet
- Intra Abdominal 2009Document8 pagesIntra Abdominal 2009Shinta Dwi Septiani Putri WibowoNo ratings yet
- Histology - Git Table 1Document1 pageHistology - Git Table 1lcrujidoNo ratings yet
- Long Case PDFDocument8 pagesLong Case PDFAbdulrahman Mohamed GhanimNo ratings yet
- Disorder of Sex DevelopmentDocument40 pagesDisorder of Sex DevelopmentAndi AdityaNo ratings yet
- 3 Surgery - Mediastinum and PleuraDocument6 pages3 Surgery - Mediastinum and PleuraCassey Koi FarmNo ratings yet
- Physical Examination of SpleenDocument5 pagesPhysical Examination of SpleenRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Arterial Blood GAS: Yrah Damiene M. Fernandez Clinical Clerk Batch 2016Document32 pagesArterial Blood GAS: Yrah Damiene M. Fernandez Clinical Clerk Batch 2016John Christopher LucesNo ratings yet
- Phlebotomy ReportDocument40 pagesPhlebotomy ReportKhelly Joshua Uy0% (1)
- History Physical FormatDocument3 pagesHistory Physical FormatfilchibuffNo ratings yet
- Mitral Valve ProlapseDocument5 pagesMitral Valve ProlapseDerofiez Hana RuhyadinNo ratings yet
- DIFFERENTIALS and MnemonicsDocument20 pagesDIFFERENTIALS and MnemonicsqurbanNo ratings yet
- Far Eastern University - Nicanor Reyes Medical FoundationDocument4 pagesFar Eastern University - Nicanor Reyes Medical FoundationMikee MeladNo ratings yet
- Bates Outline of Chapter 8Document15 pagesBates Outline of Chapter 8KatherynSotoNo ratings yet
- Clinical ExDocument123 pagesClinical ExDeepti ChaharNo ratings yet
- The Neurological ExamDocument88 pagesThe Neurological ExamsanNo ratings yet
- Core Topics in Internal MedicineDocument4 pagesCore Topics in Internal MedicineKristina Anne CoNo ratings yet
- Dse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesDocument5 pagesDse Pathogenesis/ Causes Diagnosis Complications TX Prognosis NotesLuka Desabelle- JustoNo ratings yet
- GIT Physical Examination 4th YearDocument60 pagesGIT Physical Examination 4th YearKholoud Kholoud100% (1)
- 02 1-Principles of History Taking and Physical ExaminationDocument56 pages02 1-Principles of History Taking and Physical ExaminationMorani WijegunawardanaNo ratings yet
- Clinical ExamDocument111 pagesClinical Exammuchalaith100% (2)
- YEAR 1 and 2 OSCE Revision: Author: DR Thomas PayneDocument30 pagesYEAR 1 and 2 OSCE Revision: Author: DR Thomas Payneminayoki100% (1)
- Neurology Study Guide Oral Board Exam ReviewDocument1 pageNeurology Study Guide Oral Board Exam Reviewxmc5505No ratings yet
- Cardiac Murmurs - 1p Cheat Sheet PDFDocument1 pageCardiac Murmurs - 1p Cheat Sheet PDFPkernNo ratings yet
- BRS Surgery Trauma, AbdDocument22 pagesBRS Surgery Trauma, AbdodeNo ratings yet
- OSCE Internal MedicineDocument4 pagesOSCE Internal Medicinemohamed mowafeyNo ratings yet
- Preventive CardiologyDocument28 pagesPreventive CardiologyerizonNo ratings yet
- Benign and Malignant Neoplasia of URTDocument48 pagesBenign and Malignant Neoplasia of URTsahirbuleNo ratings yet
- Clinical Exam ThyroidDocument22 pagesClinical Exam ThyroidsatyasanthiniNo ratings yet
- أدوية الطوارىءDocument162 pagesأدوية الطوارىءManar22No ratings yet
- Malassezia Furfur An-An Ap-Ap Naturally Found On The SkinDocument48 pagesMalassezia Furfur An-An Ap-Ap Naturally Found On The SkinNikki ValerioNo ratings yet
- Approach To The Patient With Endocrine DisordersDocument17 pagesApproach To The Patient With Endocrine Disordersseun williamsNo ratings yet
- Topic: Asthma and Copd: Internal Medicine IiDocument8 pagesTopic: Asthma and Copd: Internal Medicine IicarlosNo ratings yet
- Cranial Fossa Notes - HelpfulDocument4 pagesCranial Fossa Notes - HelpfulKo HakuNo ratings yet
- OSCE DermaDocument8 pagesOSCE DermaameerabestNo ratings yet
- X Ray SchemeDocument6 pagesX Ray SchemeIdiAmadouNo ratings yet
- Harrison TablesDocument5 pagesHarrison TablesSANTHILAL ADHIKARLANo ratings yet
- Chief Complaint FormatDocument3 pagesChief Complaint Formatkazniels100% (1)
- Asthma CopdDocument10 pagesAsthma CopdRem AlfelorNo ratings yet
- Cardiology Dr. Payawal UltimateDocument9 pagesCardiology Dr. Payawal UltimateSven OrdanzaNo ratings yet
- Interpretation of CBCDocument35 pagesInterpretation of CBCnth1992No ratings yet
- Neck Examination PDFDocument2 pagesNeck Examination PDFNizam Mischievous'Lovely Schremo BoyysNo ratings yet
- Mechanism of Drug Action PDFDocument1 pageMechanism of Drug Action PDFraviomjNo ratings yet
- Step-Wise Approaches in Clinical Examination - SampleDocument8 pagesStep-Wise Approaches in Clinical Examination - Samplecsbully913No ratings yet
- Medical HistoryDocument167 pagesMedical HistoryPragya Saran100% (1)
- Pericarditis 65 SlidesDocument65 pagesPericarditis 65 SlidesAtifBhoreNo ratings yet
- Cardiac InvestigationsDocument17 pagesCardiac InvestigationsTARIQ100% (1)
- CVS-01 Examination & Short CasesDocument9 pagesCVS-01 Examination & Short Casesem khanNo ratings yet
- GIT Examination - Clinical Skills With DRDocument8 pagesGIT Examination - Clinical Skills With DRNaveen KovalNo ratings yet
- Drug Toxicity and PoisoningDocument12 pagesDrug Toxicity and PoisoningPAULA MARIE MERCADO LLIDONo ratings yet
- Evaluation of Acute AbdomenDocument38 pagesEvaluation of Acute Abdomenأبو عبيدةNo ratings yet
- Scra 2014Document3 pagesScra 2014Czara DyNo ratings yet
- Republic Vs de GraciaDocument5 pagesRepublic Vs de GraciaRuiz Arenas AgacitaNo ratings yet
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyNo ratings yet
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDocument1 pageMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyNo ratings yet
- BlaaaaaaaahDocument1 pageBlaaaaaaaahCzara DyNo ratings yet
- Republic Vs de GraciaDocument5 pagesRepublic Vs de GraciaRuiz Arenas AgacitaNo ratings yet
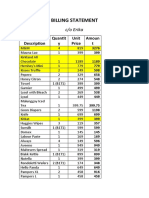
- S&R - Billing StatementDocument4 pagesS&R - Billing StatementCzara DyNo ratings yet
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyNo ratings yet
- CORPPPPPPPOOOOOOOOODocument2 pagesCORPPPPPPPOOOOOOOOOCzara DyNo ratings yet
- Castillo vs. RepublicDocument2 pagesCastillo vs. RepublicCzara DyNo ratings yet
- Lacerna Vs CorcinoDocument2 pagesLacerna Vs CorcinobenNo ratings yet
- Corpo PrelimsDocument67 pagesCorpo PrelimsCzara DyNo ratings yet
- Corpo Notes 2018 PrelimsDocument14 pagesCorpo Notes 2018 PrelimsCzara DyNo ratings yet
- Fujiki vs. MarinayDocument2 pagesFujiki vs. MarinayCzara DyNo ratings yet
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyNo ratings yet
- Garcia vs. RecioDocument2 pagesGarcia vs. RecioCzara DyNo ratings yet
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyNo ratings yet
- Banking Mon 7718Document2 pagesBanking Mon 7718Czara DyNo ratings yet
- Page 7 - 8 Proximate or Legal Cause To Legal InjuryDocument12 pagesPage 7 - 8 Proximate or Legal Cause To Legal InjuryCzara DyNo ratings yet
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyNo ratings yet
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyNo ratings yet
- Torts Finals Pages 15-19Document3 pagesTorts Finals Pages 15-19Czara DyNo ratings yet
- Sunio v. NLRCDocument3 pagesSunio v. NLRCCzara DyNo ratings yet
- Institution of Heirs. It Will Not Result To IntestacyDocument9 pagesInstitution of Heirs. It Will Not Result To IntestacyCzara DyNo ratings yet
- Jimenez vs. FranciscoDocument1 pageJimenez vs. FranciscoCzara DyNo ratings yet
- Q&A Wills Dean AligadaDocument5 pagesQ&A Wills Dean AligadaCzara DyNo ratings yet
- Evidence PPT 2018 - Dy NotesDocument14 pagesEvidence PPT 2018 - Dy NotesCzara DyNo ratings yet
- Nil Cases FinalsDocument37 pagesNil Cases FinalsCzara DyNo ratings yet
- Proximate or Legal Cause To Legal InjuryDocument12 pagesProximate or Legal Cause To Legal InjuryCzara DyNo ratings yet
- PNB Vs CA DigestDocument3 pagesPNB Vs CA DigestCzara DyNo ratings yet
- 3.0 Grand Physiology Finals Compilation - Batch 2017Document89 pages3.0 Grand Physiology Finals Compilation - Batch 2017Sheryl Layne Lao-SebrioNo ratings yet
- CG Nc2 PasserDocument28 pagesCG Nc2 PasserMary Benjie BandelariaNo ratings yet
- HEART MURMURS by NISHDocument41 pagesHEART MURMURS by NISHurtikikeNo ratings yet
- Nbme Test Taking StrategiesDocument13 pagesNbme Test Taking StrategiesSunita Shah0% (1)
- Ncma111 Lecture & Laboratory - Final: Geriatic AdaptationDocument29 pagesNcma111 Lecture & Laboratory - Final: Geriatic AdaptationBb PrintsNo ratings yet
- Heart PhysiologyDocument36 pagesHeart PhysiologyFrida Neila RahmatikaNo ratings yet
- Physical Exam Final Written Exam Study Guide 2Document51 pagesPhysical Exam Final Written Exam Study Guide 2pelly3190100% (2)
- MCQ Final Groups A, B: Attempt ReviewDocument8 pagesMCQ Final Groups A, B: Attempt ReviewYousra AhmedNo ratings yet
- Chapter 11 The Cardiovascular SystemDocument25 pagesChapter 11 The Cardiovascular SystemYeshia InocencioNo ratings yet
- Nursing: Heart DisorderDocument68 pagesNursing: Heart DisorderJhun Echipare100% (1)
- Case PresentationDocument112 pagesCase PresentationCharly Magne Tronco0% (1)
- BBS - Finals Compilation - Project Coffee PDFDocument318 pagesBBS - Finals Compilation - Project Coffee PDFNoel JoaquinNo ratings yet
- Cardio Script OSCEDocument2 pagesCardio Script OSCEbarb gNo ratings yet
- Biochemistry and Physiology Nuggets v2.1Document141 pagesBiochemistry and Physiology Nuggets v2.1fadi100% (1)
- Concise CardiologyDocument354 pagesConcise CardiologyAtish_Mathur_9874No ratings yet
- Cardiologi BookDocument287 pagesCardiologi BooknoyNo ratings yet
- Proforma For CVS History and ExaminationDocument6 pagesProforma For CVS History and ExaminationEB100% (3)
- Export Master Sheet Export Exam: Question Number: 1Document108 pagesExport Master Sheet Export Exam: Question Number: 1Moamen HellisNo ratings yet
- Propedevtika Engleski EtcDocument19 pagesPropedevtika Engleski Etcgrit27No ratings yet
- Pediatrics ImpDocument233 pagesPediatrics Impملك عيسى100% (1)
- Cardiology ExamDocument9 pagesCardiology ExamKhadar mohamedNo ratings yet
- Cardiac Physiology NotesDocument11 pagesCardiac Physiology Notespunter11100% (1)
- Heart Sounds PDFDocument38 pagesHeart Sounds PDFZennon Blaze ArceusNo ratings yet
- MCQ Int - MedDocument166 pagesMCQ Int - MedOmar Ahmed100% (1)
- Collecting Objective DataDocument61 pagesCollecting Objective DataAdrianAripNo ratings yet
- Nursing Care PlanDocument30 pagesNursing Care PlananjanaNo ratings yet
- Heart SoundDocument29 pagesHeart Sounddianpratiwirahim100% (1)
- Paeds Case Write Up 1Document29 pagesPaeds Case Write Up 1Charlotte Ee33% (3)
- Cardiology Quick Revision Final 3Document215 pagesCardiology Quick Revision Final 3bsjdbd dbNo ratings yet
- Nursing Care Plan For Heart Failure ChronicDocument26 pagesNursing Care Plan For Heart Failure ChronicbrantNo ratings yet