You might also like
- ABG Compensation InterpretationDocument2 pagesABG Compensation InterpretationLauren MarieNo ratings yet
- ECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesDocument102 pagesECG Guide: Anatomy, Physiology, Interpretation and AbnormalitiesMustafa A. DawoodNo ratings yet
- ECG Interpretation Guide for Emergency MedicineDocument39 pagesECG Interpretation Guide for Emergency MedicineAbu HibbaanNo ratings yet
- How To Take and Read An ECG ECG BasicsDocument7 pagesHow To Take and Read An ECG ECG BasicsJessica Brittain-GeorgeNo ratings yet
- Fundamentals of ECGDocument112 pagesFundamentals of ECGadithya polavarapu100% (1)
- ECG Guide: Key Components and InterpretationDocument13 pagesECG Guide: Key Components and InterpretationAllysahNo ratings yet
- Advanced EKG RefresherDocument181 pagesAdvanced EKG Refreshersimi100% (4)
- Biochemical Markers in Cardiovascular Disease: An OverviewDocument52 pagesBiochemical Markers in Cardiovascular Disease: An Overviewkarin amalia sabrina100% (1)
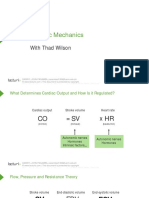
- Cardiac Mechanics: With Thad WilsonDocument26 pagesCardiac Mechanics: With Thad WilsonpasambalyrradjohndarNo ratings yet
- Usmle Hy Images: By: MeduploaderDocument62 pagesUsmle Hy Images: By: Meduploaderdamodarpatil100% (18)
- Acid-Base BalanceDocument5 pagesAcid-Base BalanceCarl Earvin L. FavoritoNo ratings yet
- Basic ECG Interpretation GuideDocument61 pagesBasic ECG Interpretation GuideHayat Hamzah DawiNo ratings yet
- Cardio Pulmo NotesDocument12 pagesCardio Pulmo NotesCherrie MaeNo ratings yet
- Electrocardiograms (ECG) : Figure 1 12 Lead ECG PerspectivesDocument8 pagesElectrocardiograms (ECG) : Figure 1 12 Lead ECG Perspectivessarb100% (1)
- Control System EbookDocument666 pagesControl System EbookNithyaa Sathish0% (1)
- ECG ECG Basics Presentation 201309101527422446 PDFDocument45 pagesECG ECG Basics Presentation 201309101527422446 PDFRamesh RajNo ratings yet
- Electrocardiography IDocument19 pagesElectrocardiography IsalochinNo ratings yet
- Basics of Chest X-RayDocument44 pagesBasics of Chest X-RayvmamikonNo ratings yet
- Hematology Oncology - Anemia ApproachDocument1 pageHematology Oncology - Anemia ApproachEugen MNo ratings yet
- ECG Circuit Analysis and Design Engineers LabsDocument29 pagesECG Circuit Analysis and Design Engineers LabsDebasish HalderNo ratings yet
- Pacemaker Sense AmplifiersDocument48 pagesPacemaker Sense AmplifiersArbab Masood AhmadNo ratings yet
- Right Side EcgDocument4 pagesRight Side EcgDragos CirsteaNo ratings yet
- Lecure-3 Biopotential ElectrodesDocument43 pagesLecure-3 Biopotential ElectrodesNoor AhmedNo ratings yet
- Principles of ECGDocument11 pagesPrinciples of ECGDeinielle Magdangal RomeroNo ratings yet
- Krishnan - EKG Basics Lecture NotesDocument3 pagesKrishnan - EKG Basics Lecture NotesanishdNo ratings yet
- NEURON ACTION POTENTIAL - PPT - ReadyDocument83 pagesNEURON ACTION POTENTIAL - PPT - Readyelle leeNo ratings yet
- NI-LabVIEW For ECG Signal ProcessingDocument5 pagesNI-LabVIEW For ECG Signal Processingamhosny64No ratings yet
- Ecg 111029102429 Phpapp01Document103 pagesEcg 111029102429 Phpapp01Vickry WahidjiNo ratings yet
- Slyt416 Ecg EegDocument18 pagesSlyt416 Ecg EegsakthyinNo ratings yet
- ECG tutorial covers basics, axis, waves, intervals, hypertrophy and moreDocument56 pagesECG tutorial covers basics, axis, waves, intervals, hypertrophy and morefeby_valNo ratings yet
- ECG MatlabDocument4 pagesECG MatlabPavan PakkiNo ratings yet
- Turning ABGs Into Childs PlayDocument35 pagesTurning ABGs Into Childs PlayLucyz KlosetNo ratings yet
- ECG LeadsDocument13 pagesECG LeadsPro fatherNo ratings yet
- Control Systems Lecture Notes Laplace TransformDocument193 pagesControl Systems Lecture Notes Laplace Transformpduff_0675% (4)
- Unit 1 Bio Potential Generation and Electrode TypesDocument13 pagesUnit 1 Bio Potential Generation and Electrode TypesAleeshaNo ratings yet
- Retrieval Tools SystemsDocument3 pagesRetrieval Tools SystemsNithyaa SathishNo ratings yet
- MRCPDocument174 pagesMRCPAbdul Quyyum100% (1)
- DAN BLS CPR Student HandbookDocument109 pagesDAN BLS CPR Student HandbookNicole Sue BucatNo ratings yet
- Blood Gas ElectrodesDocument63 pagesBlood Gas Electrodeswellawalalasith0% (1)
- MAR 2019 - MplusX QBankDocument58 pagesMAR 2019 - MplusX QBank虞君儒No ratings yet
- Icu Protocols-1Document38 pagesIcu Protocols-1M.IMRAN ANJUM100% (1)
- Blood Gas AnalyzerDocument11 pagesBlood Gas AnalyzerAleesha0% (1)
- ECG Tutorial - Basic Principles of ECG Analysis - UpToDateDocument17 pagesECG Tutorial - Basic Principles of ECG Analysis - UpToDateImja94No ratings yet
- Conquering The ECGDocument25 pagesConquering The ECGPankaj PatilNo ratings yet
- EKG Signal Processing An Algorithm To Detect and Align QRS ComplxDocument33 pagesEKG Signal Processing An Algorithm To Detect and Align QRS ComplxaryakushalNo ratings yet
- QRS Complex Detection and ECG Signal ProcessingDocument6 pagesQRS Complex Detection and ECG Signal ProcessingGoumas JimNo ratings yet
- Cardiac Action Potentials, ECG Waves & Leads ExplainedDocument11 pagesCardiac Action Potentials, ECG Waves & Leads ExplainedAndrei ManeaNo ratings yet
- Advanced Cardiac Life SupportDocument37 pagesAdvanced Cardiac Life SupportRoy Acosta GumbanNo ratings yet
- Blood Gas MachineDocument33 pagesBlood Gas MachinenofearnofearNo ratings yet
- A Brief History of Electrocardiography by Burch (Chr. Zywietz)Document10 pagesA Brief History of Electrocardiography by Burch (Chr. Zywietz)Laura Isop100% (1)
- Image processing of ECG wave using MatlabDocument21 pagesImage processing of ECG wave using MatlabrakeshNo ratings yet
- Lecure-5 The Origin of Biopotentials - 2Document34 pagesLecure-5 The Origin of Biopotentials - 2Noor Ahmed100% (1)
- Approach To DyspneaDocument9 pagesApproach To DyspneaMuhammad LukmanNo ratings yet
- Medical Electronics Question BankDocument3 pagesMedical Electronics Question BankmathavanNo ratings yet
- Unit 2: Biosignal Characteristics and Electrode ConfigurationsDocument34 pagesUnit 2: Biosignal Characteristics and Electrode ConfigurationsEZHIL NNo ratings yet
- Matlab Code For EcgDocument5 pagesMatlab Code For Ecgsriteja406No ratings yet
- PharmacologyDocument120 pagesPharmacologyFluffy_iceNo ratings yet
- A Simplified ECG GuideDocument4 pagesA Simplified ECG GuideMarian Ioan-LucianNo ratings yet
- 3-EEG Fni$Document50 pages3-EEG Fni$chanlalNo ratings yet
- Design and Implementation of a 12-Channel ECG DeviceDocument74 pagesDesign and Implementation of a 12-Channel ECG DeviceMcSudul HasanNo ratings yet
- Arterial Blood Gas.Document4 pagesArterial Blood Gas.Sathish KumarNo ratings yet
- Medical Analyzers Spec2017Document21 pagesMedical Analyzers Spec2017Carlos Matallana100% (1)
- CARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFDocument40 pagesCARDIAC ELECTROPHYSIOLOGY AND THE ELECTROCARDIOGRAM - ClinicalKey PDFMelanie DascăluNo ratings yet
- Pacemaker Output Circuit Design for Optimal Patient StimulationDocument30 pagesPacemaker Output Circuit Design for Optimal Patient StimulationVishwanath ShervegarNo ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- Module 1 Questions and AnswersDocument2 pagesModule 1 Questions and AnswersAmberNo ratings yet
- Problems of Discussion: Nonlinear Analysis of ECG: A Noninvasive Way of Medical DiagnosisDocument48 pagesProblems of Discussion: Nonlinear Analysis of ECG: A Noninvasive Way of Medical DiagnosisNur HossainNo ratings yet
- Νευρολογία σύνολο απαντήσεωνDocument38 pagesΝευρολογία σύνολο απαντήσεωνCheng Kuao HengNo ratings yet
- Ecg Physio LectureDocument60 pagesEcg Physio LectureAninze Chidera100% (1)
- REAL Time ECG TRAINER MANUALDocument15 pagesREAL Time ECG TRAINER MANUALSHANKARNo ratings yet
- ECGDocument15 pagesECGJegathese BaskerNo ratings yet
- Types of WheelchairsDocument13 pagesTypes of WheelchairsMehnaz KhanNo ratings yet
- Design of Artificial Arms and Hands For Prosthetic ApplicationsDocument28 pagesDesign of Artificial Arms and Hands For Prosthetic ApplicationsNithyaa SathishNo ratings yet
- Hilbert-Huang Transform and Its Applications in Engineering and Biomedical Signal AnalysisDocument8 pagesHilbert-Huang Transform and Its Applications in Engineering and Biomedical Signal AnalysisNithyaa SathishNo ratings yet
- EGGDocument14 pagesEGGNithyaa SathishNo ratings yet
- 1 s2.0 S1607551X11001835 MainDocument13 pages1 s2.0 S1607551X11001835 MainNithyaa SathishNo ratings yet
- Telehealth (MX9014)Document2 pagesTelehealth (MX9014)Nithyaa SathishNo ratings yet
- Respiratory Mechanics and Gas ExchangeDocument14 pagesRespiratory Mechanics and Gas ExchangeNithyaa SathishNo ratings yet
- Diabetic Foot Ulcers - Prevention, Diagnosis and Classification - American Family PhysicianDocument6 pagesDiabetic Foot Ulcers - Prevention, Diagnosis and Classification - American Family PhysicianNithyaa SathishNo ratings yet
- New Electric Prosthetic System with Simultaneous Elbow & Hand ControlDocument10 pagesNew Electric Prosthetic System with Simultaneous Elbow & Hand ControlNithyaa SathishNo ratings yet
- Pattern NotesDocument23 pagesPattern NotesArchanaBmeNo ratings yet
- Part BDocument2 pagesPart BNithyaa SathishNo ratings yet
- Webb CHPT 6s4Document14 pagesWebb CHPT 6s4aloove66No ratings yet
- Encryption MatlabDocument9 pagesEncryption MatlabKaris Shang100% (1)
- ElectronicsDocument8 pagesElectronicsNithyaa SathishNo ratings yet
- Automated Detection and Classification of Parasitic and Non-Parasitic DiseasesDocument12 pagesAutomated Detection and Classification of Parasitic and Non-Parasitic DiseasesNithyaa SathishNo ratings yet
- Radiopharmaceuticals For Radioisotope ImagingDocument21 pagesRadiopharmaceuticals For Radioisotope ImagingNithyaa SathishNo ratings yet
- ch54MEASUREMENT TECHNIQUES IN RESPIRATORY MECHANICSDocument16 pagesch54MEASUREMENT TECHNIQUES IN RESPIRATORY MECHANICSNithyaa SathishNo ratings yet
- Mathematical Modeling of Respiratory System: A ReviewDocument5 pagesMathematical Modeling of Respiratory System: A ReviewNithyaa SathishNo ratings yet
- Bonus Chapt 07Document36 pagesBonus Chapt 07Niki KarmannNo ratings yet
- Therapeutic Indication Ofelectrohomeopathic MedicinesDocument8 pagesTherapeutic Indication Ofelectrohomeopathic MedicinesMeghanath PandhikondaNo ratings yet
- AUBF Serous FluidDocument7 pagesAUBF Serous FluidRichelyn Grace B. VenusNo ratings yet
- Anemia - Ferrum MetDocument6 pagesAnemia - Ferrum MetManali JainNo ratings yet
- Liver Anatomy and Physiology ReviewDocument4 pagesLiver Anatomy and Physiology ReviewLen Bernabe RuizNo ratings yet
- Cardiovascular System: Dulay, Arjay SDocument21 pagesCardiovascular System: Dulay, Arjay SarjayNo ratings yet
- Nicole Michaela Rillo Midterms Patient CaseDocument18 pagesNicole Michaela Rillo Midterms Patient CaseKyla TuanNo ratings yet
- Resting ECG Report FormDocument1 pageResting ECG Report FormKarthik SNo ratings yet
- Case Study 1Document3 pagesCase Study 1Da NicaNo ratings yet
- Medical Terminogy: Assignment - 1Document5 pagesMedical Terminogy: Assignment - 1Vineet SinghNo ratings yet
- Pancreatic Enzymes Help Digest CarbsDocument7 pagesPancreatic Enzymes Help Digest CarbsAngelaAmmcoNo ratings yet
- Peer Reviewed Medical Papers Submitted To Various Medical Journals, Evidencing A Multitude of Adverse Events in Covid-19 Vaccine RecipientsDocument77 pagesPeer Reviewed Medical Papers Submitted To Various Medical Journals, Evidencing A Multitude of Adverse Events in Covid-19 Vaccine RecipientsKraft DinnerNo ratings yet
- Hypertension-Linked Kidney DamageDocument4 pagesHypertension-Linked Kidney Damagerichelle cortesNo ratings yet
- Tetralogy of FallotDocument61 pagesTetralogy of FallotHanya BelajarNo ratings yet
- Jurnal 11Document7 pagesJurnal 11Zella ZakyaNo ratings yet
- CVA JroozDocument5 pagesCVA JroozEdmonLagartoNo ratings yet
- Review Assessment Quiz 1 Ischemic StrokeDocument4 pagesReview Assessment Quiz 1 Ischemic Strokelcastro8No ratings yet
- Pejie Ann Cornites Analou O. Hermocilla Haydee C. Diola: Rosario P. PoleaDocument10 pagesPejie Ann Cornites Analou O. Hermocilla Haydee C. Diola: Rosario P. PoleaERNESTO MARAVILLANo ratings yet
- WWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteDocument16 pagesWWW - Medicalppt.: For More Free Medical Powerpoint Presentations Visit WebsiteSujith RaoNo ratings yet
- Recent Advances in Cerebral PalsyDocument16 pagesRecent Advances in Cerebral PalsyTasyaNo ratings yet
- Slide Referensi Natexam 2018Document54 pagesSlide Referensi Natexam 2018Sellyta HasugianNo ratings yet
- 4 5787572421108171420 PDFDocument62 pages4 5787572421108171420 PDFnanda1al1humairahNo ratings yet