You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Left, The Right, and The State (Read in "Fullscreen")Document570 pagesThe Left, The Right, and The State (Read in "Fullscreen")Ludwig von Mises Institute100% (68)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- AMEE and BEME GuidesDocument10 pagesAMEE and BEME GuidesaungNo ratings yet
- AMEE and BEME GuidesDocument10 pagesAMEE and BEME GuidesaungNo ratings yet
- AMEE and BEME GuidesDocument10 pagesAMEE and BEME GuidesaungNo ratings yet
- The Failure To Prevent Genocide in Rwanda The Role of BystandersDocument329 pagesThe Failure To Prevent Genocide in Rwanda The Role of BystandersAlexandra CiarnauNo ratings yet
- Valuing Human Capital at Infosys Using Lev & Schwartz ModelDocument3 pagesValuing Human Capital at Infosys Using Lev & Schwartz ModelAnchal Jain100% (2)
- 9 STRDocument8 pages9 STRaungNo ratings yet
- 11 Passage 2Document2 pages11 Passage 2aungNo ratings yet
- PCR ssp1Document4 pagesPCR ssp1aungNo ratings yet
- Bmi Asia Pasifik PDFDocument4 pagesBmi Asia Pasifik PDFFarid NurdiansyahNo ratings yet
- Burning TestDocument1 pageBurning TestaungNo ratings yet
- Denaturing PAGE GelDocument2 pagesDenaturing PAGE GelaungNo ratings yet
- Arm Touch 60 Brochure v2Document2 pagesArm Touch 60 Brochure v2aungNo ratings yet
- Investigating Race and Ethnicity On Data Collection and AnalysisDocument7 pagesInvestigating Race and Ethnicity On Data Collection and AnalysisaungNo ratings yet
- Compact Family Gel Electrophoresis SystemsDocument5 pagesCompact Family Gel Electrophoresis SystemsaungNo ratings yet
- Amplified DNA Product Separation For Forensic AnalystsDocument24 pagesAmplified DNA Product Separation For Forensic AnalystsaungNo ratings yet
- Advancing Medical Education - The New Series of AMEE Guides in Medical EducationDocument2 pagesAdvancing Medical Education - The New Series of AMEE Guides in Medical EducationaungNo ratings yet
- (A. J. Jeffreys, S. D. J. Pena (Auth.), Prof. Dr.Document453 pages(A. J. Jeffreys, S. D. J. Pena (Auth.), Prof. Dr.aungNo ratings yet
- PUFADocument5 pagesPUFAaungNo ratings yet
- AMEE Guide No. 11 (Revised) - Portfolio-Based Learning and Assessment in Medical EducationDocument17 pagesAMEE Guide No. 11 (Revised) - Portfolio-Based Learning and Assessment in Medical EducationaungNo ratings yet
- AMEE Guide No. 5 The Core Curriculum With Options or Special Study ModulesDocument24 pagesAMEE Guide No. 5 The Core Curriculum With Options or Special Study ModulesaungNo ratings yet
- AMEE Guide No. 4 Effective Continuing Education - The CRISIS CriteriaDocument16 pagesAMEE Guide No. 4 Effective Continuing Education - The CRISIS CriteriaaungNo ratings yet
- HormonesDocument5 pagesHormonesaungNo ratings yet
- AMEE Guide No. 6 Evaluating Multimedia Applications For Medical EducationDocument12 pagesAMEE Guide No. 6 Evaluating Multimedia Applications For Medical EducationaungNo ratings yet
- Get2 2 PDFDocument74 pagesGet2 2 PDFaungNo ratings yet
- Con PhilDocument48 pagesCon PhilConica BurgosNo ratings yet
- Family Law Final Exam ReviewDocument2 pagesFamily Law Final Exam ReviewArielleNo ratings yet
- Online Applicaiton Regulations Under CQ (MBBS&BDS) ChangedDocument23 pagesOnline Applicaiton Regulations Under CQ (MBBS&BDS) Changedyamini susmitha PNo ratings yet
- ERP in Apparel IndustryDocument17 pagesERP in Apparel IndustrySuman KumarNo ratings yet
- SIBUR - 1H 2020 - Results - PresentationDocument22 pagesSIBUR - 1H 2020 - Results - Presentation757rustamNo ratings yet
- ACC WagesDocument4 pagesACC WagesAshish NandaNo ratings yet
- Social media types for media literacyDocument28 pagesSocial media types for media literacyMa. Shantel CamposanoNo ratings yet
- Narrative On Parents OrientationDocument2 pagesNarrative On Parents Orientationydieh donaNo ratings yet
- Church Sacraments SlideshareDocument19 pagesChurch Sacraments SlidesharelimmasalustNo ratings yet
- Micro - Welfare EconomicsDocument14 pagesMicro - Welfare EconomicsTanvi ShahNo ratings yet
- Overtime Request Form 加班申请表: Last Name First NameDocument7 pagesOvertime Request Form 加班申请表: Last Name First NameOlan PrinceNo ratings yet
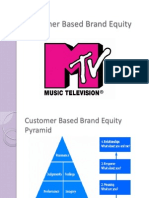
- Customer Based Brand EquityDocument13 pagesCustomer Based Brand EquityZeeshan BakshiNo ratings yet
- Battle of Qadisiyyah: Muslims defeat Sassanid PersiansDocument22 pagesBattle of Qadisiyyah: Muslims defeat Sassanid PersiansMustafeez TaranNo ratings yet
- Esp 7 Q4M18Document13 pagesEsp 7 Q4M18Ellecarg Cenaon CruzNo ratings yet
- PEST Analysis of the Indian Pharmaceutical IndustryDocument8 pagesPEST Analysis of the Indian Pharmaceutical IndustryAnkush GuptaNo ratings yet
- Meeting Consumers ' Connectivity Needs: A Report From Frontier EconomicsDocument74 pagesMeeting Consumers ' Connectivity Needs: A Report From Frontier EconomicsjkbuckwalterNo ratings yet
- Marine Insurance Final ITL & PSMDocument31 pagesMarine Insurance Final ITL & PSMaeeeNo ratings yet
- Case Study Format Hvco Srce UhvDocument2 pagesCase Study Format Hvco Srce Uhvaayushjn290No ratings yet
- Personal Values: Definitions & TypesDocument1 pagePersonal Values: Definitions & TypesGermaeGonzalesNo ratings yet
- Techm Work at Home Contact Center SolutionDocument11 pagesTechm Work at Home Contact Center SolutionRashi ChoudharyNo ratings yet
- Sweetlines v. TevesDocument6 pagesSweetlines v. TevesSar FifthNo ratings yet
- International Buffet Menu Rm45.00Nett Per Person Appertizer and SaladDocument3 pagesInternational Buffet Menu Rm45.00Nett Per Person Appertizer and SaladNorasekin AbdullahNo ratings yet
- Olsson Jah ResilienceDocument12 pagesOlsson Jah ResilienceANA ZABRINA PERDOMO MERLOSNo ratings yet
- Applied Crypto HardeningDocument111 pagesApplied Crypto Hardeningadr99No ratings yet
- HB Nutrition FinalDocument14 pagesHB Nutrition FinalJaoNo ratings yet
- Language Teacher Educator IdentityDocument92 pagesLanguage Teacher Educator IdentityEricka RodriguesNo ratings yet
- Regulatory Framework in Business Transactions: Law On PartnershipDocument16 pagesRegulatory Framework in Business Transactions: Law On PartnershipDan DiNo ratings yet