You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Papulas y Placas Pruriginosas Bialteral AuricularDocument3 pagesPapulas y Placas Pruriginosas Bialteral AuricularAntonio MoncadaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 2016 Vitiligo Mbe CochraneDocument8 pages2016 Vitiligo Mbe CochraneAntonio MoncadaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Tto Asma CronicaDocument15 pagesTto Asma CronicaAntonio MoncadaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hipertension Pulmonar DX y TtoDocument7 pagesHipertension Pulmonar DX y TtoAntonio MoncadaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- DX Clinico de Gota Sin Aspiracion de ArticulacionDocument2 pagesDX Clinico de Gota Sin Aspiracion de ArticulacionAntonio MoncadaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Ivermectina 1% RosaceaDocument2 pagesIvermectina 1% RosaceaAntonio MoncadaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CroupDocument3 pagesCroupAntonio MoncadaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- P 114Document7 pagesP 114Sleepy WinterNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- AAFP Feb 2016 Bleeding and BruisingDocument8 pagesAAFP Feb 2016 Bleeding and BruisingAntonio MoncadaNo ratings yet
- Antitrombotico Oral 2013 GuiaDocument2 pagesAntitrombotico Oral 2013 GuiaAntonio MoncadaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Breats PDFDocument5 pagesBreats PDFAntonio MoncadaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Anticoagulan TherpayDocument17 pagesAnticoagulan TherpayCh RoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Convulsion Febril - Febrile Seizures Risks, Evaluation, and Prognosis - Am Fam Physician. 2012Document5 pagesConvulsion Febril - Febrile Seizures Risks, Evaluation, and Prognosis - Am Fam Physician. 2012Nataly Zuluaga VilladaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Colitis Ulverativa 2013Document7 pagesColitis Ulverativa 2013Antonio MoncadaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Diagnosis and Treatment of AcneDocument7 pagesDiagnosis and Treatment of AcnenovialbarNo ratings yet
- Addison 2014 PDFDocument6 pagesAddison 2014 PDFAntonio MoncadaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Set 2016-Sind Apnea Obst SueñoDocument7 pagesSet 2016-Sind Apnea Obst SueñoAntonio MoncadaNo ratings yet
- Screening Depresion Uspstf - Agosto 2016Document4 pagesScreening Depresion Uspstf - Agosto 2016Antonio MoncadaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- AAFP 2016 Febrero - Anemia en NiñosDocument9 pagesAAFP 2016 Febrero - Anemia en NiñosAntonio MoncadaNo ratings yet
- AAFP Sarcoidosis 2016Document11 pagesAAFP Sarcoidosis 2016Antonio MoncadaNo ratings yet
- Set 2016-Antihistaminicos h1 2da Generaiocn-Urticaria CronicaDocument2 pagesSet 2016-Antihistaminicos h1 2da Generaiocn-Urticaria CronicaAntonio MoncadaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- AAFP Ago 2016 Retraso en El DesarrolloDocument6 pagesAAFP Ago 2016 Retraso en El DesarrolloAntonio MoncadaNo ratings yet
- Rinosinusitis - Agosto 2016Document9 pagesRinosinusitis - Agosto 2016Antonio MoncadaNo ratings yet
- AAFP Jul 2016 DX y Manejo de FX VertebralDocument7 pagesAAFP Jul 2016 DX y Manejo de FX VertebralAntonio MoncadaNo ratings yet
- AAFP Marzo 2016 HipertiroidismoDocument11 pagesAAFP Marzo 2016 HipertiroidismoAntonio MoncadaNo ratings yet
- Sind Ovario Poliquistico 2016 - NejmDocument11 pagesSind Ovario Poliquistico 2016 - NejmAntonio MoncadaNo ratings yet
- Neuropatia Diabetica Periferica Agosto 2016Document8 pagesNeuropatia Diabetica Periferica Agosto 2016Antonio MoncadaNo ratings yet
- 283 FullDocument11 pages283 FullWelki VernandoNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- BLS & AclsDocument29 pagesBLS & AclswcgokulNo ratings yet
- Ebstein AnomalyDocument14 pagesEbstein AnomalyNataliaMaedyNo ratings yet
- Rohini 59284010117Document21 pagesRohini 59284010117narasimmanbiomedicalNo ratings yet
- Raza's ECGDocument45 pagesRaza's ECGcozmoxxxNo ratings yet
- 500 Single Best Answers in MedicineDocument443 pages500 Single Best Answers in MedicineOmar Ahmed100% (1)
- 10 CardiomyopathyDocument71 pages10 CardiomyopathyAnonymous vUEDx8100% (5)
- Electrocardiogram: Dr. PacnaDocument13 pagesElectrocardiogram: Dr. PacnaEcel AggasidNo ratings yet
- Caring For A Patient After Coronary Artery Bypass.6Document6 pagesCaring For A Patient After Coronary Artery Bypass.6Nadia BeadleNo ratings yet
- Cardio PDFDocument94 pagesCardio PDFSalwaNo ratings yet
- 2.500548 Medilog Holter System PP en LQDocument8 pages2.500548 Medilog Holter System PP en LQIvan CvasniucNo ratings yet
- AF Catheter AblationDocument37 pagesAF Catheter AblationSnehal JayaramNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Leadership & Management Management ConceptsDocument94 pagesLeadership & Management Management Conceptsamasoud96 amasoud96No ratings yet
- Arrhythmia Overview: Antonia Anna LukitoDocument45 pagesArrhythmia Overview: Antonia Anna LukitoJoshua ObrienNo ratings yet
- CSI Chennai 2016 Highlights PDFDocument190 pagesCSI Chennai 2016 Highlights PDFmohamedsmnNo ratings yet
- Hemiplegia Resource Book ModifiedDocument60 pagesHemiplegia Resource Book ModifiedAnonymous czrvb3hNo ratings yet
- B009HQA92MDocument520 pagesB009HQA92Mrama DulalNo ratings yet
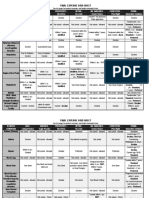
- Final Expense Cheat SheetDocument15 pagesFinal Expense Cheat Sheetapi-622084072No ratings yet
- Vasopressor & InotropeDocument29 pagesVasopressor & InotropeAl Hijjah FadhilahNo ratings yet
- Palpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Document19 pagesPalpitation:evaluation, Ambulatory Monitoring, Mobile Telemetry Eg - MCOT@2012Navojit ChowdhuryNo ratings yet
- Group 13, Case 1 Neuro AssignmentDocument9 pagesGroup 13, Case 1 Neuro AssignmentRajat DeyNo ratings yet
- Uptodte TSVDocument215 pagesUptodte TSVcrilala23No ratings yet
- Hypertensive Heart Disease: A Proposed Clinical ClassificationDocument2 pagesHypertensive Heart Disease: A Proposed Clinical ClassificationRonald Hamdani HamNo ratings yet
- Book of AbstractsDocument38 pagesBook of Abstractssome bodyNo ratings yet
- Nclex Question and Rationale - Week 2Document9 pagesNclex Question and Rationale - Week 2ShiraishiNo ratings yet
- Fuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary ADocument33 pagesFuster Et Al 2001 Acc Aha Esc Guidelines For The Management of Patients With Atrial Fibrillation Executive Summary AAlfita RahmawatiNo ratings yet
- Cardiac Intensive Care Unit Admission CriteriaDocument19 pagesCardiac Intensive Care Unit Admission CriteriaVina Tri AdityaNo ratings yet
- Atrial Fibrillation PresentationDocument22 pagesAtrial Fibrillation PresentationZulyusri GhazaliNo ratings yet
- FLASHCARD CardiovascularDocument40 pagesFLASHCARD CardiovascularsnehaNo ratings yet
- Primary Care Medicine Office Evaluation and Management of The Adult Patient Ebook PDF VersionDocument62 pagesPrimary Care Medicine Office Evaluation and Management of The Adult Patient Ebook PDF Versionthelma.brown536100% (41)
- Yoga For The Heart EbookDocument38 pagesYoga For The Heart EbookYogaBasics100% (3)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (29)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (2)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (81)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)