You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Definition of NephrolithiasisDocument30 pagesDefinition of Nephrolithiasiszz_13No ratings yet
- Lesson 1Document20 pagesLesson 1Irish Jean AgsawayNo ratings yet
- Cardiology Case 1Document2 pagesCardiology Case 1vil62650% (2)
- Significance of Facebow Transfer: January 2020Document6 pagesSignificance of Facebow Transfer: January 2020Mahmoud Ibrahem maanNo ratings yet
- Physioex Lab Report: Pre-Lab Quiz ResultsDocument4 pagesPhysioex Lab Report: Pre-Lab Quiz ResultsNovanza RayhanNo ratings yet
- Mini-implant molar intrusion caseDocument1 pageMini-implant molar intrusion caseVesna AndreevskaNo ratings yet
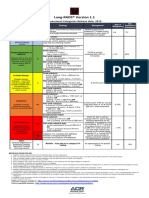
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- Acute Kidney Injury W/ Hyperkalemia NCPDocument5 pagesAcute Kidney Injury W/ Hyperkalemia NCPMyrvic Ortiz La OrdenNo ratings yet
- Lesson 3 ReviewDocument4 pagesLesson 3 ReviewHo Yong WaiNo ratings yet
- Anterior Cruciate Ligament InjuryDocument3 pagesAnterior Cruciate Ligament InjuryAdrian Nazario PragachaNo ratings yet
- Jomi 7657Document27 pagesJomi 7657casto.carpetasmiaNo ratings yet
- Expression of MDM2 and p16 in AngiomyolipomaDocument7 pagesExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresNo ratings yet
- Infectiile Grave Extensive Ale Partilor MoiDocument49 pagesInfectiile Grave Extensive Ale Partilor MoiLoredana BoghezNo ratings yet
- HomeostasisDocument12 pagesHomeostasisTimothy StanleyNo ratings yet
- Ligibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineDocument20 pagesLigibel JA Et Al. 2022 Exercise, Diet and Weight Management During Cancer Treatment - ASCO GuidelineJasmyn KimNo ratings yet
- Askep CKD Bhs InggrisDocument15 pagesAskep CKD Bhs InggrisFitri MulyaNo ratings yet
- Important Classifications PDFDocument42 pagesImportant Classifications PDF330 Himank MehtaNo ratings yet
- Anticestodal Drugs for Tapeworm TreatmentDocument3 pagesAnticestodal Drugs for Tapeworm TreatmentAbiHa YousaufNo ratings yet
- Health and IllnessDocument2 pagesHealth and IllnessLize Decotelli HubnerNo ratings yet
- Asthma Attack Nursing Care Plan for Married Female PatientDocument5 pagesAsthma Attack Nursing Care Plan for Married Female PatientMarivic Yuson MalagarNo ratings yet
- Prostaglandins: An Overview of Structure and FunctionDocument33 pagesProstaglandins: An Overview of Structure and FunctionMuhammad JamalNo ratings yet
- List of Empanelled Hospitals in CGHS NagpurDocument58 pagesList of Empanelled Hospitals in CGHS NagpurRajatNo ratings yet
- History of HIVDocument4 pagesHistory of HIVHyrum KamandeNo ratings yet
- US Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreDocument4 pagesUS Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreWilmer Zambrano GuerreroNo ratings yet
- Oral Health During Pregnancy - An Analysis of Information CoDocument8 pagesOral Health During Pregnancy - An Analysis of Information CoElena IancuNo ratings yet
- Role of Autologous Platelet-Rich Plasma in Z-PlastyDocument3 pagesRole of Autologous Platelet-Rich Plasma in Z-PlastyasclepiuspdfsNo ratings yet
- Foot reflexology chart shows how hand acupressure points relate to body partsDocument3 pagesFoot reflexology chart shows how hand acupressure points relate to body partsgautamlipika100% (2)
- Source Control in Emergency General SurgeryDocument21 pagesSource Control in Emergency General SurgerylaviniaNo ratings yet
- Abnormal PuerperiumDocument65 pagesAbnormal PuerperiumNigus AfessaNo ratings yet
- Dental Public HealthDocument264 pagesDental Public HealthCorina Manole DanielaNo ratings yet