You might also like
- Pacs CondaDocument7 pagesPacs CondaSpiriidione PuzzarNo ratings yet
- Pacs CondaDocument7 pagesPacs CondaSpiriidione PuzzarNo ratings yet
- App Whit PythonDocument74 pagesApp Whit PythonSpiriidione PuzzarNo ratings yet
- Slez 012Document2 pagesSlez 012Spiriidione PuzzarNo ratings yet
- Relay Timer BRDDocument1 pageRelay Timer BRDSpiriidione PuzzarNo ratings yet
- Arduino - ArduinoToBreadboardDocument3 pagesArduino - ArduinoToBreadboardSpiriidione PuzzarNo ratings yet
- How Can I Practice A Specific Opening?: FAQ Written by BolokayDocument28 pagesHow Can I Practice A Specific Opening?: FAQ Written by BolokayjohnNo ratings yet
- sn75176b PDFDocument25 pagessn75176b PDFSpiriidione PuzzarNo ratings yet
- Slez 012Document2 pagesSlez 012Spiriidione PuzzarNo ratings yet
- xx555 Precision Timers: 1 Features 3 DescriptionDocument36 pagesxx555 Precision Timers: 1 Features 3 DescriptionHanen MejbriNo ratings yet
- HP01DDocument6 pagesHP01DSpiriidione PuzzarNo ratings yet
- PCM 2902 BDocument33 pagesPCM 2902 BSpiriidione PuzzarNo ratings yet
- ASROCK 775i65gDocument38 pagesASROCK 775i65gPhilip Lorenzana ReytiranNo ratings yet
- FLOW080LDocument2 pagesFLOW080LSpiriidione PuzzarNo ratings yet
- Savant DigiFlow 6710M Digital Water Flow MeterDocument3 pagesSavant DigiFlow 6710M Digital Water Flow MeterSpiriidione PuzzarNo ratings yet
- Resultados ZaidaDocument3 pagesResultados ZaidaSpiriidione PuzzarNo ratings yet
- FLOW40L0Document2 pagesFLOW40L0Spiriidione PuzzarNo ratings yet
- Savant FS-2000H Flow SensorDocument3 pagesSavant FS-2000H Flow SensorSpiriidione PuzzarNo ratings yet
- Normal RankDocument1 pageNormal RankSpiriidione PuzzarNo ratings yet
- Resultados ZaidaDocument3 pagesResultados ZaidaSpiriidione PuzzarNo ratings yet
- Referencias 01.1.2012Document37 pagesReferencias 01.1.2012Spiriidione PuzzarNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Abinisio GDE HelpDocument221 pagesAbinisio GDE HelpvenkatesanmuraliNo ratings yet
- Cianura Pentru Un Suras de Rodica OjogDocument1 pageCianura Pentru Un Suras de Rodica OjogMaier MariaNo ratings yet
- Modified Release Drug ProductsDocument58 pagesModified Release Drug Productsmailtorubal2573100% (2)
- Antiquity: Middle AgesDocument6 pagesAntiquity: Middle AgesPABLO DIAZNo ratings yet
- AAU5243 DescriptionDocument30 pagesAAU5243 DescriptionWisut MorthaiNo ratings yet
- Insize Catalogue 2183,2392Document1 pageInsize Catalogue 2183,2392calidadcdokepNo ratings yet
- Reservoir Rock TypingDocument56 pagesReservoir Rock TypingAffan HasanNo ratings yet
- USA V BRACKLEY Jan6th Criminal ComplaintDocument11 pagesUSA V BRACKLEY Jan6th Criminal ComplaintFile 411No ratings yet
- The Singular Mind of Terry Tao - The New York TimesDocument13 pagesThe Singular Mind of Terry Tao - The New York TimesX FlaneurNo ratings yet
- All Associates Warning Against ChangesDocument67 pagesAll Associates Warning Against Changesramesh0% (1)
- Major Bank Performance IndicatorsDocument35 pagesMajor Bank Performance IndicatorsAshish MehraNo ratings yet
- Modern Indian HistoryDocument146 pagesModern Indian HistoryJohn BoscoNo ratings yet
- Colour Ring Labels for Wireless BTS IdentificationDocument3 pagesColour Ring Labels for Wireless BTS Identificationehab-engNo ratings yet
- Steps To Configure Linux For Oracle 9i Installation: 1. Change Kernel ParametersDocument5 pagesSteps To Configure Linux For Oracle 9i Installation: 1. Change Kernel ParametersruhelanikNo ratings yet
- JSA - 0026 Chipping & Granite cutting and lying Work At PB-19Document2 pagesJSA - 0026 Chipping & Granite cutting and lying Work At PB-19Koneti JanardhanaraoNo ratings yet
- Lecture 4Document25 pagesLecture 4ptnyagortey91No ratings yet
- 2002, Vol.86, Issues 4, Hospital MedicineDocument221 pages2002, Vol.86, Issues 4, Hospital MedicineFaisal H RanaNo ratings yet
- Key ssl101 Academic Skills For University Success ssl101cDocument196 pagesKey ssl101 Academic Skills For University Success ssl101cHùng NguyễnNo ratings yet
- Cisco CMTS Feature GuideDocument756 pagesCisco CMTS Feature GuideEzequiel Mariano DaoudNo ratings yet
- Miami Police File The O'Nell Case - Clemen Gina D. BDocument30 pagesMiami Police File The O'Nell Case - Clemen Gina D. Barda15biceNo ratings yet
- Ecole Polytechnique Federale de LausanneDocument44 pagesEcole Polytechnique Federale de LausanneSyed Yahya HussainNo ratings yet
- Honors Biology Unit 2 - Energy Study GuideDocument2 pagesHonors Biology Unit 2 - Energy Study GuideMark RandolphNo ratings yet
- 2016 Mustang WiringDocument9 pages2016 Mustang WiringRuben TeixeiraNo ratings yet
- APC Smart-UPS 1500VA LCD 230V: Part Number: SMT1500IDocument3 pagesAPC Smart-UPS 1500VA LCD 230V: Part Number: SMT1500IDesigan SannasyNo ratings yet
- VL2019201000534 DaDocument2 pagesVL2019201000534 DaEnjoy LifeNo ratings yet
- PWC Global Project Management Report SmallDocument40 pagesPWC Global Project Management Report SmallDaniel MoraNo ratings yet
- Department of Education: Weekly Home Learning Plan Grade Ii Fourth Quarter Week 8Document8 pagesDepartment of Education: Weekly Home Learning Plan Grade Ii Fourth Quarter Week 8Evelyn DEL ROSARIONo ratings yet
- PREMIUM BINS, CARDS & STUFFDocument4 pagesPREMIUM BINS, CARDS & STUFFSubodh Ghule100% (1)
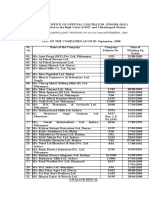
- Statement of Compulsory Winding Up As On 30 SEPTEMBER, 2008Document4 pagesStatement of Compulsory Winding Up As On 30 SEPTEMBER, 2008abchavhan20No ratings yet
- Jazan Refinery and Terminal ProjectDocument3 pagesJazan Refinery and Terminal ProjectkhsaeedNo ratings yet