You might also like
- Fisiologi Hati Dan Kandung EmpeduDocument24 pagesFisiologi Hati Dan Kandung EmpeduMusmul AlqorubNo ratings yet
- Pemeriksaan Radiologi Pada Trauma GinjalDocument21 pagesPemeriksaan Radiologi Pada Trauma GinjalQotrunnada Alwi Zubaidah, S.KedNo ratings yet
- Typhoid Management Guidelines - 2019 - MMIDSPDocument14 pagesTyphoid Management Guidelines - 2019 - MMIDSPhasnah shintaNo ratings yet
- Biuret TestDocument10 pagesBiuret TestJanine Vega Calayo100% (1)
- Ulkus PeptikumDocument30 pagesUlkus PeptikumRizky Indah SorayaNo ratings yet
- Patofisiologi Sistem PerkemihanDocument24 pagesPatofisiologi Sistem PerkemihanMasna Arisah NasutionNo ratings yet
- Kuliah BMD Pathomechanism DemaDocument30 pagesKuliah BMD Pathomechanism DemaSelebriti Indonesia100% (1)
- Sindrom NefrotikDocument22 pagesSindrom NefrotikGyta Apriati100% (1)
- Makalah 4 CMLDocument28 pagesMakalah 4 CMLMentari100% (1)
- Cardiac Biomarker 2014Document41 pagesCardiac Biomarker 2014flower boyNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- HotLab Agustus 2019-DikonversiDocument71 pagesHotLab Agustus 2019-DikonversiEndy JuliantoNo ratings yet
- Jurnal Urinalisis - Kelompok 4Document8 pagesJurnal Urinalisis - Kelompok 4Ekello Michael WaasNo ratings yet
- n378.008 Iris Website Staging of CKD PDFDocument8 pagesn378.008 Iris Website Staging of CKD PDFrutebeufNo ratings yet
- Regulasi Dan Mekanisme EndokrinDocument121 pagesRegulasi Dan Mekanisme Endokrinluthfiyya syafiqaNo ratings yet
- Thrombotic Thrombocytopenic Purpura (TTP) : Rd. Kemas Diffa Zahputra. PKDocument11 pagesThrombotic Thrombocytopenic Purpura (TTP) : Rd. Kemas Diffa Zahputra. PKAnonymous cy6fLANo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Pharmacology of Antipyretic DrugsDocument19 pagesPharmacology of Antipyretic DrugsPretty HiaNo ratings yet
- Difusi AgarDocument5 pagesDifusi AgarOkiSutantoNo ratings yet
- Atlas of Diseases of The KidneyDocument1,095 pagesAtlas of Diseases of The KidneyYanka IlarionovaNo ratings yet
- Natrium BikarbonatDocument5 pagesNatrium BikarbonatUlly AmriNo ratings yet
- PDF DipiroDocument16 pagesPDF DipiroYolandaFandraIINo ratings yet
- IsotonisDocument27 pagesIsotonisIllhaa AlvielhaaNo ratings yet
- Kuliah Keseimbangan Asam BasaDocument38 pagesKuliah Keseimbangan Asam BasaSarah Lesty Adila100% (1)
- Hipofise & HipothalamusDocument44 pagesHipofise & HipothalamusvaliamnisaNo ratings yet
- Jurnal GlikogenDocument6 pagesJurnal GlikogenChoirummintin Wa KhilafahNo ratings yet
- Jurnal - Olopatadine HCL Vs Ketotifen Fumarate Untuk Konjungtivitis AlergiDocument19 pagesJurnal - Olopatadine HCL Vs Ketotifen Fumarate Untuk Konjungtivitis AlergiPutriIffahNo ratings yet
- Guidelines For The Management of Hemophilia: 2 EditionDocument80 pagesGuidelines For The Management of Hemophilia: 2 EditionMuhammad BilalNo ratings yet
- 5a. Mekanisme Imunitas Seluler Dan HumoralDocument32 pages5a. Mekanisme Imunitas Seluler Dan HumoralGaluh Apsari SyafranNo ratings yet
- EritrositDocument12 pagesEritrositNatasya HerinNo ratings yet
- GUS1 - K5 - Renal Blood Flow and Glomerular FiltrationDocument23 pagesGUS1 - K5 - Renal Blood Flow and Glomerular FiltrationRudinNo ratings yet
- Diagnosis & Tata Laksana Cad / CcsDocument40 pagesDiagnosis & Tata Laksana Cad / CcsIno HajrinNo ratings yet
- Modified Release Per Oral Dosage FormDocument43 pagesModified Release Per Oral Dosage FormNurRohmanNo ratings yet
- An Introduction: Distillation Is Defined AsDocument15 pagesAn Introduction: Distillation Is Defined AsVeronica_Dewi_2361No ratings yet
- Farmakokinetika Tugas Soal PPT EkstravaskulerDocument17 pagesFarmakokinetika Tugas Soal PPT Ekstravaskulertaka oneokrock18No ratings yet
- The Cardiovascular System: The Heart: AnatomyDocument62 pagesThe Cardiovascular System: The Heart: AnatomyLingga GumelarNo ratings yet
- Antihistamine PresentationDocument34 pagesAntihistamine PresentationOpa Evilsiam100% (1)
- Renal Calculi & Renal FailureDocument17 pagesRenal Calculi & Renal Failureazlan100% (1)
- Anemia Penyakit KronikDocument12 pagesAnemia Penyakit KronikFaridhatulNo ratings yet
- Anatomi Dan Fisiologi PerkemihanDocument89 pagesAnatomi Dan Fisiologi Perkemihannia djNo ratings yet
- Terjemahan Jurnal FeDocument19 pagesTerjemahan Jurnal FeNadiaa RamadhaniNo ratings yet
- Metabolism: CHEM 2066Document31 pagesMetabolism: CHEM 2066karlo100% (1)
- PhysioEx Exercise 4 Activity 2Document3 pagesPhysioEx Exercise 4 Activity 2PatriNo ratings yet
- KP 1.3.2.3 Fisiologi Sistem Saraf PeriferDocument50 pagesKP 1.3.2.3 Fisiologi Sistem Saraf PeriferShintia Surya PutriNo ratings yet
- Surfactant PresentationDocument18 pagesSurfactant PresentationMaadaNo ratings yet
- 2016 PAD ACC+AHA SlidesDocument74 pages2016 PAD ACC+AHA SlidesPonpimol Odee BongkeawNo ratings yet
- Dr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik UnjaDocument18 pagesDr. Ave Olivia Rahman, Msc. Bagian Farmakologi Fkik Unjariska yulizaNo ratings yet
- Mineral Homeostasis BoneDocument20 pagesMineral Homeostasis BoneSawsan Z. JwaiedNo ratings yet
- HIPERVOLEMIADocument22 pagesHIPERVOLEMIAperkakas78No ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaIndrasti BanjaransariNo ratings yet
- Farmakologi Obat Hemostasis & AntikoagulanDocument19 pagesFarmakologi Obat Hemostasis & AntikoagulanamirahNo ratings yet
- Kokristal ParasetamolDocument6 pagesKokristal Parasetamolslmkhns46No ratings yet
- Edema: Pendrik Tandean Internal Medicine, Medical Faculty of Hasanuddin University, MakassarDocument31 pagesEdema: Pendrik Tandean Internal Medicine, Medical Faculty of Hasanuddin University, MakassarLIEBERKHUNNo ratings yet
- Methacholine1 21Document21 pagesMethacholine1 21Mihaela Dudau100% (1)
- United States Court of Appeals, Fourth CircuitDocument5 pagesUnited States Court of Appeals, Fourth CircuitScribd Government DocsNo ratings yet
- Kuliah 5. Kasus 1 Dan 2 (GGK)Document94 pagesKuliah 5. Kasus 1 Dan 2 (GGK)yudiNo ratings yet
- Congestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCDocument25 pagesCongestive Heart Failure (CHF) / Decompensation Cordis Functional Class (DCFCYUSRIL ZUMADINSYAHNo ratings yet
- Timebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisFrom EverandTimebomb:The Global Epidemic of Multi-Drug Resistant TuberculosisRating: 3.5 out of 5 stars3.5/5 (2)
- Rational Use of Diawdawduretic and Patofisiologi EdemaDocument10 pagesRational Use of Diawdawduretic and Patofisiologi EdemaWendy WiharjaNo ratings yet
- Hyponatremia in Cirrhosis: An Update: Joseph J. Alukal, MD, Savio John, MD and Paul J. Thuluvath, MD, FRCPDocument11 pagesHyponatremia in Cirrhosis: An Update: Joseph J. Alukal, MD, Savio John, MD and Paul J. Thuluvath, MD, FRCPMuzaffar MehdiNo ratings yet
- Diuretics: DR Mozna TalpurDocument33 pagesDiuretics: DR Mozna TalpurShahid HameedNo ratings yet
- Case Study: A Patient With Type 2 Diabetes Working With An Advanced Practice Pharmacist To Address Interacting ComorbiditiesDocument8 pagesCase Study: A Patient With Type 2 Diabetes Working With An Advanced Practice Pharmacist To Address Interacting ComorbiditiessamanNo ratings yet
- Jurnal Penatalaksanaan EdemaDocument7 pagesJurnal Penatalaksanaan EdemaMariska Nada Debora100% (1)
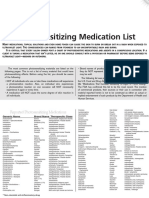
- Photosensitizing Medication ListDocument3 pagesPhotosensitizing Medication ListDimas RfNo ratings yet
- Farmakoterapi Sistem RenalDocument89 pagesFarmakoterapi Sistem RenalNhovieNhowaaNo ratings yet
- Drug StudyDocument19 pagesDrug StudyCalimlim KimNo ratings yet
- Naplex ReviewDocument63 pagesNaplex Reviewdivinevalley100% (7)
- Diuretics: Generic and Brand NamesDocument22 pagesDiuretics: Generic and Brand NamesKish GabrielNo ratings yet
- Renal System PPT (Pharmacology)Document100 pagesRenal System PPT (Pharmacology)Cheska DillupacNo ratings yet
- Drugs Affecting The Renal System I. Diuretics II. Parenteral Fluids (Video) III. Electrolytes (Video)Document44 pagesDrugs Affecting The Renal System I. Diuretics II. Parenteral Fluids (Video) III. Electrolytes (Video)Juliene Hannah FloresNo ratings yet
- My Revision Qs - Huda MadanliDocument18 pagesMy Revision Qs - Huda MadanliSandeep KannegantiNo ratings yet
- Integrated Therapeutics-Ii For 3 Year STS: Chapter-1Document69 pagesIntegrated Therapeutics-Ii For 3 Year STS: Chapter-1Geleta GalataaNo ratings yet
- For The Clinician: Clinical Pharmacology in Diuretic UseDocument10 pagesFor The Clinician: Clinical Pharmacology in Diuretic UseSrinivas PingaliNo ratings yet
- Calvin Damanik, DR, SPPD: Departement Penyakit Dalam Fak Kedokteran Umi MedDocument37 pagesCalvin Damanik, DR, SPPD: Departement Penyakit Dalam Fak Kedokteran Umi MedMaria lestari harianjaNo ratings yet
- Case Study-Congestive Heart FailureDocument71 pagesCase Study-Congestive Heart FailureKentTangcalagan92% (13)
- Pharmacy Formulary - Booklet - 2016Document178 pagesPharmacy Formulary - Booklet - 2016pcartercNo ratings yet
- Diuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutDocument33 pagesDiuretics: BY-DR. Saurabh Kansal Dept. of Pharmacology Msy Medical College MeerutPrakhar GoelNo ratings yet
- Hypertension: Dr. Isbandiyah, SPPD FK UmmDocument41 pagesHypertension: Dr. Isbandiyah, SPPD FK UmmSemestaNo ratings yet
- Natural Medicines Comprehensive Database 2010Document26 pagesNatural Medicines Comprehensive Database 2010PsineticNo ratings yet
- Questions KatzungDocument46 pagesQuestions KatzungYalman Eyinç100% (3)
- HF PresentationDocument62 pagesHF Presentationapi-552486649No ratings yet
- نسخة Pharma1 diuretics and anti HTN. Manar.BQDocument6 pagesنسخة Pharma1 diuretics and anti HTN. Manar.BQAblah Hamdan ThaherNo ratings yet
- Cardiac Drugs HypertensionDocument5 pagesCardiac Drugs HypertensionEciOwnsMeNo ratings yet
- 2016 ATC Index With DDDDocument317 pages2016 ATC Index With DDDSi CentilNo ratings yet
- DiureticsDocument10 pagesDiureticsAyla NacariøNo ratings yet
- 7896 - Super NAPLEX Review PDFDocument72 pages7896 - Super NAPLEX Review PDFFrancis Leonardes100% (8)
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYC100% (2)
- Acute Heart Failure WORKBOOKDocument28 pagesAcute Heart Failure WORKBOOKFadhlan ABNo ratings yet
- LicoriceDocument11 pagesLicoricelinaNo ratings yet
- "Natriuresis": Prepared by Dr. Hala Zaqout 1Document89 pages"Natriuresis": Prepared by Dr. Hala Zaqout 1Ahmed FouadNo ratings yet