You might also like
- A Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Adrenal Cancer, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Hyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHyper-coagulation, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Surgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal GlandsDocument38 pagesSurgical Pathology For Dentistry Students - Surgical Pathology of Thyroid and Adrenal Glandssorin niky mocanu100% (1)
- Triglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Document20 pagesTriglycerides and VLDL: (Increased Ra Tio of Triglyceride To Apob)Indah Pujiati DtNo ratings yet
- Pathology Parathyroid GlandsDocument14 pagesPathology Parathyroid GlandsEman KhammasNo ratings yet
- Drug-induced Liver Disease (DILD) Causes, Types, DiagnosisDocument30 pagesDrug-induced Liver Disease (DILD) Causes, Types, DiagnosisSurya PratamaNo ratings yet
- Laboratory Diagnostics of (Selected) Endocrine DisordersDocument48 pagesLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteNo ratings yet
- Family-Oriented Primary CareDocument16 pagesFamily-Oriented Primary CareMwanja MosesNo ratings yet
- Evaluation of Liver FunctionDocument64 pagesEvaluation of Liver FunctionMustafa KhandgawiNo ratings yet
- The Yale Way - New Patient PresentationsDocument9 pagesThe Yale Way - New Patient PresentationsAndrew McGowanNo ratings yet
- Interpreting Thyroid Tests: Key FactorsDocument7 pagesInterpreting Thyroid Tests: Key FactorsStrawberry ShortcakeNo ratings yet
- Hemodiafiltration Kuhlmann PDFDocument31 pagesHemodiafiltration Kuhlmann PDFDavid SantosoNo ratings yet
- Project B EdDocument17 pagesProject B EdAnju VijayanNo ratings yet
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 pagesMedical Case 1: Language Centre of Malahayati University at 2010putri1114No ratings yet
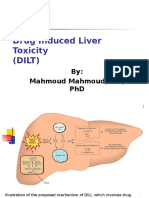
- Drug Induced Liver Toxicity (DILT): Mechanisms, Classifications and SpectrumDocument39 pagesDrug Induced Liver Toxicity (DILT): Mechanisms, Classifications and SpectrumAjeng SekariniNo ratings yet
- Lymphoma (Ean's) - 2Document29 pagesLymphoma (Ean's) - 2eanfital11No ratings yet
- Borderline Personality Disorder Diagnosis Symptoms TreatmentDocument57 pagesBorderline Personality Disorder Diagnosis Symptoms TreatmentAnand KirtiNo ratings yet
- Pre AnaestheticsDocument69 pagesPre AnaestheticsPraney SlathiaNo ratings yet
- Chemo PrinciplesDocument3 pagesChemo PrinciplesSze Hui OoiNo ratings yet
- Chemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Document57 pagesChemical Pathology Workshop II - Diagnostic Theory in Chemical Pathology (2017.11.14)Arthur Chang100% (1)
- Abdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccDocument38 pagesAbdul Rahim Bin Mohamad Nor C 111 10 871: Prof - Dr.Peter Kabo, PHD, SPFK, SPJP (K), Fiha, FasccAis KonorasNo ratings yet
- Duodenal AtresiaDocument18 pagesDuodenal AtresiaRianto Noviady RamliNo ratings yet
- Particular Cancer Power PointDocument101 pagesParticular Cancer Power PointKoRnflakesNo ratings yet
- Thyroid NodulesDocument34 pagesThyroid NodulesEphobiaNo ratings yet
- 1.05 Liver and Portal HypertensionDocument12 pages1.05 Liver and Portal HypertensionZazaNo ratings yet
- Physical Diagnosis - The Art of History TakingDocument3 pagesPhysical Diagnosis - The Art of History TakingCassandra Doyaoen100% (1)
- Stem Cell TransplantationDocument13 pagesStem Cell TransplantationMylls MondejarNo ratings yet
- Managing HIV Patients & HAART Metabolic ComplicationsDocument33 pagesManaging HIV Patients & HAART Metabolic ComplicationsSimeon AdebisiNo ratings yet
- Necrotizing Fasciitis..By DR Kassahun GirmaDocument49 pagesNecrotizing Fasciitis..By DR Kassahun GirmaKassahun Girma GelawNo ratings yet
- Testicular CancerDocument48 pagesTesticular Cancerluckyswiss7776848No ratings yet
- Endocrinology HandbookDocument75 pagesEndocrinology Handbookhirsi200518No ratings yet
- Approach To HematuriaDocument45 pagesApproach To HematuriaArun GeorgeNo ratings yet
- Evaluation of Chest Pain: Ruling Out Life ThreatsDocument16 pagesEvaluation of Chest Pain: Ruling Out Life ThreatsAbhinit RiddhiNo ratings yet
- Step Up To Medicine 2004Document1,259 pagesStep Up To Medicine 2004Mariana GomezNo ratings yet
- Cervical Cancer Screening and DiagnosisDocument137 pagesCervical Cancer Screening and DiagnosisBhattarai ShrinkhalaNo ratings yet
- Interpret Liver TestsDocument4 pagesInterpret Liver TestsKaram Ali ShahNo ratings yet
- Drug ToxicityDocument21 pagesDrug ToxicityUsman Akhtar0% (1)
- RBC Degradation & Causes of JaundiceDocument30 pagesRBC Degradation & Causes of JaundiceSubhi MishraNo ratings yet
- Hyperprolactine MIA: Prepared By: Daryl S. AbrahamDocument15 pagesHyperprolactine MIA: Prepared By: Daryl S. AbrahamBiway RegalaNo ratings yet
- Lower Female Genital Tract InfectionsDocument42 pagesLower Female Genital Tract InfectionsAwal Sher khanNo ratings yet
- Thyroid Disease AlgorithmsDocument29 pagesThyroid Disease AlgorithmsGoh Chong Aik100% (1)
- Vasopressors and Inotropes in ShockDocument8 pagesVasopressors and Inotropes in ShockRiska PashaNo ratings yet
- Metastatic Pancreatic CancerDocument16 pagesMetastatic Pancreatic CancerJorge Osorio100% (1)
- Extrahepatic CholestasisDocument31 pagesExtrahepatic CholestasismackieccNo ratings yet
- Antibiotic SlideDocument56 pagesAntibiotic SlidePhongsathorn PhlaisaithongNo ratings yet
- 2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)Document7 pages2D2016 3.4-2 Azotemia and Urinary Abnormalities (Harrison's)elleinas100% (1)
- Cushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyDocument25 pagesCushing'S Syndrome: Roldan, Scorch Dominique Romero, John Reden Sanchez, Tracy JoyGerald John PazNo ratings yet
- Ascites PresentationDocument19 pagesAscites PresentationDanielle FosterNo ratings yet
- Severe Sepsis and Septic Shock in EDDocument31 pagesSevere Sepsis and Septic Shock in EDtarrynwortmann5319No ratings yet
- CCT - CCI Code of EthicsDocument2 pagesCCT - CCI Code of EthicsAvanca LouisNo ratings yet
- Cellular PathologyDocument58 pagesCellular PathologyRKNo ratings yet
- General Principles of Combination ChemotherapyDocument40 pagesGeneral Principles of Combination Chemotherapyoncology KMC-KnlNo ratings yet
- Plasmapheresis For AutoimmunityDocument14 pagesPlasmapheresis For AutoimmunityEliDavidNo ratings yet
- Haematology New20format20 2007Document9 pagesHaematology New20format20 2007Valter VascainoNo ratings yet
- Risk Factors: About Breast CancerDocument5 pagesRisk Factors: About Breast CancerShyamol Bose100% (1)
- Control of Blood Tissue Blood Flow: Faisal I. Mohammed, MD, PHDDocument25 pagesControl of Blood Tissue Blood Flow: Faisal I. Mohammed, MD, PHDManohar SinghNo ratings yet
- Palliative CareDocument4 pagesPalliative CareJohn Rex Baltazar Jr.No ratings yet
- Hormon GDSDocument23 pagesHormon GDSBRI KUNo ratings yet
- Inflamed Aorta, (Aortitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandInflamed Aorta, (Aortitis) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Salivary Gland Cytology: A Color AtlasFrom EverandSalivary Gland Cytology: A Color AtlasMousa A. Al-AbbadiRating: 5 out of 5 stars5/5 (2)
- The Computer Based Patient Record An Essential Technology For Health Care Revised Edition PDFDocument257 pagesThe Computer Based Patient Record An Essential Technology For Health Care Revised Edition PDFرونالين كسترو100% (1)
- 03 Yukiasha Den (Fushigi Yuugi Gaiden 3 - Nuriko)Document155 pages03 Yukiasha Den (Fushigi Yuugi Gaiden 3 - Nuriko)api-3706651100% (10)
- Dealing With DistressDocument42 pagesDealing With Distresspanickedchick100% (2)
- Dealing With DistressDocument42 pagesDealing With Distresspanickedchick100% (2)
- Pseudo RelationshipDocument3 pagesPseudo Relationshipرونالين كستروNo ratings yet
- Mulan Saves China by Disguising Herself as a ManDocument6 pagesMulan Saves China by Disguising Herself as a Manرونالين كستروNo ratings yet
- Pseudo RelationshipDocument3 pagesPseudo Relationshipرونالين كستروNo ratings yet
- Tumor StagingDocument9 pagesTumor Stagingmalaran.deboraheloisaNo ratings yet
- Review Test Unit 7-8-1 Akhir KunjawDocument10 pagesReview Test Unit 7-8-1 Akhir KunjawSakya RyoukaNo ratings yet
- Oral Hygiene Care PlanDocument2 pagesOral Hygiene Care PlanMisaelMonteroGarridoNo ratings yet
- Agriculture, biotech, bioethics challenges of globalized food systemsDocument28 pagesAgriculture, biotech, bioethics challenges of globalized food systemsperoooNo ratings yet
- Medical BacteriologyDocument108 pagesMedical BacteriologyTamarah YassinNo ratings yet
- Maternal Serum Alpha-Fetoprotein (MSAFP)Document2 pagesMaternal Serum Alpha-Fetoprotein (MSAFP)Shaells JoshiNo ratings yet
- Abilify Drug Study: Therapeutic Effects, Indications, Contraindications and Adverse ReactionsDocument6 pagesAbilify Drug Study: Therapeutic Effects, Indications, Contraindications and Adverse ReactionsLuige AvilaNo ratings yet
- Eneza Ujumbe: The Voices of Mathare YouthDocument4 pagesEneza Ujumbe: The Voices of Mathare YouthakellewagumaNo ratings yet
- Oral Glucose Tolerance TestDocument4 pagesOral Glucose Tolerance TestCyna Jane Yao AlcularNo ratings yet
- I VC GuidelinesDocument22 pagesI VC Guidelinesganesha trengginasNo ratings yet
- The So Called Oedematous Skin DiseaseDocument22 pagesThe So Called Oedematous Skin Diseaseمحمد على أحمد أحمدNo ratings yet
- Debabrata Paper Vol-1-No.-1-Article-10Document5 pagesDebabrata Paper Vol-1-No.-1-Article-10Debabrata PariaNo ratings yet
- Templates For Planning and M&E (AIP, WFP, SMEA Templates)Document6 pagesTemplates For Planning and M&E (AIP, WFP, SMEA Templates)Genzo TaniaNo ratings yet
- Laws of Malaysia: Act A1648Document42 pagesLaws of Malaysia: Act A1648ana rizanNo ratings yet
- Laws and policies against cigarette smokingDocument16 pagesLaws and policies against cigarette smokingHarlene Dela Cruz OzarNo ratings yet
- Hyperglycemia in PregnancyDocument17 pagesHyperglycemia in PregnancyIza WidzNo ratings yet
- HFpEF Management 2023Document10 pagesHFpEF Management 2023ctsakalakisNo ratings yet
- Public Availability of Labeling CBE Guidance PDFDocument6 pagesPublic Availability of Labeling CBE Guidance PDFMichael wangNo ratings yet
- BBA Enrollment Form Front Page PDFDocument2 pagesBBA Enrollment Form Front Page PDFYaj EstefanoNo ratings yet
- Psychological Disorders Chapter OutlineDocument13 pagesPsychological Disorders Chapter OutlineCameron PhillipsNo ratings yet
- Jejunostomy Feeding Tube Placement in GastrectomyDocument14 pagesJejunostomy Feeding Tube Placement in GastrectomyHarshit UdaiNo ratings yet
- Full Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFDocument41 pagesFull Download Ebook Ebook PDF Nelson Essentials of Pediatrics 8th Edition PDFdavid.anderson198100% (37)
- hw320 Unit 9 Final Assigment Stacey StoryDocument15 pageshw320 Unit 9 Final Assigment Stacey Storyapi-651674228No ratings yet
- Path122 Diabetes MellitusDocument12 pagesPath122 Diabetes MellitusGwendolaine PicaNo ratings yet
- Care of Normal Newborn BabiesDocument439 pagesCare of Normal Newborn BabiesSebastian Spatariu100% (2)
- PEH 11 Q3 Mod1 Week 1 2 MELC01 Thelma R. SacsacDocument16 pagesPEH 11 Q3 Mod1 Week 1 2 MELC01 Thelma R. Sacsaccalvin adralesNo ratings yet
- Pediatrics in Review - March2011Document67 pagesPediatrics in Review - March2011Manuel Alvarado50% (2)
- Neo JaundiceDocument67 pagesNeo Jaundicemanisha thakur100% (1)
- A Message From Dauphin County Chairman Jeff Haste To Citizens of PADocument2 pagesA Message From Dauphin County Chairman Jeff Haste To Citizens of PAPennLiveNo ratings yet
- Understanding Literature SynthesisDocument5 pagesUnderstanding Literature SynthesisJimboy MaglonNo ratings yet