You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lipoma in Submandibular Region - A Case ReportDocument4 pagesLipoma in Submandibular Region - A Case Reportmaxfac2010No ratings yet
- Full Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFDocument41 pagesFull Download Book Microbiome Immunity Digestive Health and Nutrition Epidemiology Pathophysiology Prevention and Treatment PDFmildred.walker324100% (15)
- IFAD Vietnam RIMS Training Workshop 2011 (1 of 7)Document18 pagesIFAD Vietnam RIMS Training Workshop 2011 (1 of 7)IFAD VietnamNo ratings yet
- Sebuguero V NLRC Case Digest PDFDocument2 pagesSebuguero V NLRC Case Digest PDFYodh Jamin Ong0% (1)
- Catalog en Eurocoustic 0Document132 pagesCatalog en Eurocoustic 0Vikash KumarNo ratings yet
- Leader Ship Assessment: Student No 374212036Document4 pagesLeader Ship Assessment: Student No 374212036Emily KimNo ratings yet
- Genius 7 On Bill Acceptor ManualDocument10 pagesGenius 7 On Bill Acceptor ManualJose Maria PerezNo ratings yet
- Fourier Ptychography Stivi ElbiDocument20 pagesFourier Ptychography Stivi ElbistiviNo ratings yet
- AlaTOP Allergy Screen OUS - IMMULITE 2000 Systems - Rev 21 DXDCM 09017fe98067cfcb-1645658153157Document28 pagesAlaTOP Allergy Screen OUS - IMMULITE 2000 Systems - Rev 21 DXDCM 09017fe98067cfcb-1645658153157Pierre LavoisierNo ratings yet
- Static Fluid: It Is Mass Per Unit Volume at Certain TemperatureDocument11 pagesStatic Fluid: It Is Mass Per Unit Volume at Certain TemperatureMohamed El-GoharyNo ratings yet
- Manual Servicio Soxte 2050Document46 pagesManual Servicio Soxte 2050Quimica JordanlabNo ratings yet
- Presentation On Heavy Engineering Corporation LimitedDocument20 pagesPresentation On Heavy Engineering Corporation LimitedSandeepRajNo ratings yet
- The Emerging Field of Emotion Regulation - An Integrative Review - James J GrossDocument29 pagesThe Emerging Field of Emotion Regulation - An Integrative Review - James J GrossLely AprianiNo ratings yet
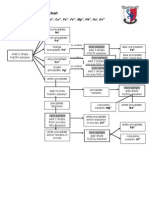
- Testing For Cations Flow ChartDocument2 pagesTesting For Cations Flow Chartapi-252561013No ratings yet
- Soal Uh English XDocument1 pageSoal Uh English XhenniherawatiNo ratings yet
- What Is A Walkable Place The Walkability Debate inDocument20 pagesWhat Is A Walkable Place The Walkability Debate inBADR HAMDAN ALATEBENo ratings yet
- Leadership 29Document32 pagesLeadership 29Efe AgbozeroNo ratings yet
- Stern TubesDocument8 pagesStern Tubesweesweekwee8652No ratings yet
- Connection Manual: BNP-B2203D (ENG)Document122 pagesConnection Manual: BNP-B2203D (ENG)Allison CarvalhoNo ratings yet
- MSW TACSOP v.3.3Document59 pagesMSW TACSOP v.3.3Mira BellaNo ratings yet
- CS1 Epoxy Curing AgentsDocument21 pagesCS1 Epoxy Curing AgentsAlptekin100% (1)
- 2013 Medigate Profile PDFDocument26 pages2013 Medigate Profile PDFGabriel Duran DiazNo ratings yet
- Daily 500 Maximum 2500 Minimum 1000 Lead Time 15 Days EOQ 1200 Emergency Lead Time 3 DaysDocument5 pagesDaily 500 Maximum 2500 Minimum 1000 Lead Time 15 Days EOQ 1200 Emergency Lead Time 3 DaysM Noaman AkbarNo ratings yet
- Adobeconstruct 19 NeubDocument34 pagesAdobeconstruct 19 NeublailanuitNo ratings yet
- VW Golf 8 Variant WD EngDocument664 pagesVW Golf 8 Variant WD EngLakhdar BouchenakNo ratings yet
- A211 Reading Set A QuestionDocument12 pagesA211 Reading Set A Questiontasya zakariaNo ratings yet
- What Is Primary Health Care and Its Relation To Universal Health Care? As A Medical Student, What Impact Can I Create in Implementing PHC and UHC?Document2 pagesWhat Is Primary Health Care and Its Relation To Universal Health Care? As A Medical Student, What Impact Can I Create in Implementing PHC and UHC?Aubrey Unique EvangelistaNo ratings yet
- Biological Activity of Bone Morphogenetic ProteinsDocument4 pagesBiological Activity of Bone Morphogenetic Proteinsvanessa_werbickyNo ratings yet
- Ableism - What It Is and Why It Matters To EveryoneDocument28 pagesAbleism - What It Is and Why It Matters To Everyonellemma admasNo ratings yet
- Total Parenteral NutritionDocument8 pagesTotal Parenteral NutritionTemiloluwa AdeyemiNo ratings yet