You might also like
- Submitted By:: Vaniya Ravikumar G. REG NO: 2010118141 Plant Pathology 2 SEMESTER M.Sc. (Agri) N.M.C.A, N.A.U, NAVSARIDocument13 pagesSubmitted By:: Vaniya Ravikumar G. REG NO: 2010118141 Plant Pathology 2 SEMESTER M.Sc. (Agri) N.M.C.A, N.A.U, NAVSARIRAMESH CHAUDHARYNo ratings yet
- Trichoderma Harzianum by Clyde Chloe D. TrayaDocument5 pagesTrichoderma Harzianum by Clyde Chloe D. TrayaLouie PalaraoNo ratings yet
- Philippine HMO Ruling on DST Tax ExemptionDocument4 pagesPhilippine HMO Ruling on DST Tax ExemptionJian CerreroNo ratings yet
- Economics of Cacao Production in KonaDocument12 pagesEconomics of Cacao Production in KonaHarlin AvestruzNo ratings yet
- Villa V GArciaDocument3 pagesVilla V GArciaCharismaPerezNo ratings yet
- Annex 13 - CocoaPhilDocument4 pagesAnnex 13 - CocoaPhilaseancocoaclubNo ratings yet
- 050 - Autocorp V IntraDocument3 pages050 - Autocorp V IntraVM MIGNo ratings yet
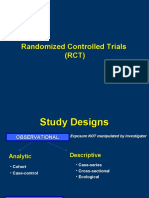
- RCT Study DesignsDocument47 pagesRCT Study DesignsbramNo ratings yet
- Marine ProtestDocument2 pagesMarine ProtestZyreen Kate CataquisNo ratings yet
- Sales - Finals (Digests)Document10 pagesSales - Finals (Digests)oniksukkieNo ratings yet
- 243 MFS Tire and Rubber, Inc. v. CADocument3 pages243 MFS Tire and Rubber, Inc. v. CAEdvin HitosisNo ratings yet
- Datoon Vs Judge KapiliDocument2 pagesDatoon Vs Judge KapiliTenet ManzanoNo ratings yet
- Sterling Products Vs Sol (Feb 28, 1963)Document2 pagesSterling Products Vs Sol (Feb 28, 1963)mNo ratings yet
- Why Closed-Shop Provisions Cannot Be Applied RetroactivelyDocument2 pagesWhy Closed-Shop Provisions Cannot Be Applied RetroactivelyBen Dover McDuffins100% (1)
- LaborRev Handwritten CasesDocument16 pagesLaborRev Handwritten Casesejusdem generis100% (1)
- Host Plant ResistanceDocument8 pagesHost Plant ResistanceSyafinaz WanNo ratings yet
- NORECO1 Appeals Dismissal of Petition Challenging Certification of UnionDocument4 pagesNORECO1 Appeals Dismissal of Petition Challenging Certification of UnionArbie Mae SalomaNo ratings yet
- PAL Vs Civil Aeronautics BoardDocument1 pagePAL Vs Civil Aeronautics BoardBeverlyn JamisonNo ratings yet
- Hacienda Luisita Case Digest July Nov Apr PDFDocument7 pagesHacienda Luisita Case Digest July Nov Apr PDFArwella GregorioNo ratings yet
- Sandiganbayan Jurisdiction Over Officers of Government-Owned CorporationsDocument7 pagesSandiganbayan Jurisdiction Over Officers of Government-Owned CorporationsMp CasNo ratings yet
- CSC V AppealDocument3 pagesCSC V Appealjeth saganaNo ratings yet
- Divine Word High School Vs NLRCDocument3 pagesDivine Word High School Vs NLRCVince LeidoNo ratings yet
- Motion For Postponement - Elena LlantoDocument2 pagesMotion For Postponement - Elena LlantoSalvado and Chua Law OfficesNo ratings yet
- Ruga Vs NLRCDocument1 pageRuga Vs NLRCRobert QuiambaoNo ratings yet
- Labor Union Fees DisputeDocument2 pagesLabor Union Fees DisputeChino SisonNo ratings yet
- RA No 8792Document10 pagesRA No 8792Lizzy WayNo ratings yet
- Baseline Survey On The Status, Family and Socio-Economic Status of Persons With Disabilities in Bawku West District (GHANA)Document110 pagesBaseline Survey On The Status, Family and Socio-Economic Status of Persons With Disabilities in Bawku West District (GHANA)Monaliza Calapini-PrasadNo ratings yet
- Sanyo Philippines Workers Union-PSSLU Vs Canizares: FactsDocument7 pagesSanyo Philippines Workers Union-PSSLU Vs Canizares: FactsDon VillegasNo ratings yet
- Rice Insect Pest Management Ecological ConceptsDocument52 pagesRice Insect Pest Management Ecological ConceptsJames LitsingerNo ratings yet
- Tricho Derma As BioDocument14 pagesTricho Derma As BiovioindahNo ratings yet
- 60 Day Freedom Period - COLLECTIVE BARGAINING AGREEMENTDocument7 pages60 Day Freedom Period - COLLECTIVE BARGAINING AGREEMENTArmandM.TaacaNo ratings yet
- (G.R. No. 170007. April 7, 2014.) Tabangao Shell Refinery Employees Association, Petitioner, vs. Pilipinas Shell Petroleum CORPORATION, RespondentDocument3 pages(G.R. No. 170007. April 7, 2014.) Tabangao Shell Refinery Employees Association, Petitioner, vs. Pilipinas Shell Petroleum CORPORATION, RespondentEkie Gonzaga100% (1)
- Apelario vs. Ines Chavez & CoDocument4 pagesApelario vs. Ines Chavez & CoAsHervea AbanteNo ratings yet
- Nat'l Congress of Unions in The Sugar Industry vs. Trajano GR No. L-67485Document5 pagesNat'l Congress of Unions in The Sugar Industry vs. Trajano GR No. L-67485King KingNo ratings yet
- Coca Cola Bottlers Vs Ilocos ProfessionalDocument2 pagesCoca Cola Bottlers Vs Ilocos ProfessionalRewel Jr. MedicoNo ratings yet
- GR 107019 Drilon V CADocument9 pagesGR 107019 Drilon V CAAyvee BlanchNo ratings yet
- Mapa v. Ca 275 Scra 286Document10 pagesMapa v. Ca 275 Scra 286Kurisuchan DamnitNo ratings yet
- A-IPRA V Comelec PDFDocument2 pagesA-IPRA V Comelec PDFDominic EstremosNo ratings yet
- R. Transport Corporation vs. Laguesma - DIGDocument3 pagesR. Transport Corporation vs. Laguesma - DIGbananayellowsharpieNo ratings yet
- Ford Philippines Marketing PlanDocument15 pagesFord Philippines Marketing PlanJames Lee IlaganNo ratings yet
- Co-Op Rural Bank of Davao V Ferrer-CallejaDocument7 pagesCo-Op Rural Bank of Davao V Ferrer-CallejaAngelo0% (1)
- Case Digests Labor RelationsDocument30 pagesCase Digests Labor RelationsAmanda ButtkissNo ratings yet
- Furusawa Rubber Phil Vs Sec of LaborDocument3 pagesFurusawa Rubber Phil Vs Sec of LaborJMF1234No ratings yet
- Oscar Gaboa VS Maunlad Trans, Inc PDFDocument16 pagesOscar Gaboa VS Maunlad Trans, Inc PDFkristel jane caldozaNo ratings yet
- BSU College of Law Thesis on SurrogacyDocument5 pagesBSU College of Law Thesis on SurrogacyRiffy OisinoidNo ratings yet
- San Juan de Dios Hospital vs. NLRC 282 SCRA 316, 1997 FactsDocument2 pagesSan Juan de Dios Hospital vs. NLRC 282 SCRA 316, 1997 FactsHoreb FelixNo ratings yet
- PCIB and NestleDocument7 pagesPCIB and NestleRENZO NIÑO ROSALESNo ratings yet
- Liberal Party vs. ComelecDocument25 pagesLiberal Party vs. ComelecheyoooNo ratings yet
- UPLB Trichoderma Biotech - CuevasDocument5 pagesUPLB Trichoderma Biotech - CuevasArt Esmeralda100% (1)
- Apex Mining V Southeast Mindanao Gold Mining EscraDocument44 pagesApex Mining V Southeast Mindanao Gold Mining EscraEd ManzanoNo ratings yet
- Gaoiran VS. Alcala, 444 SCRA 428 (2005)Document6 pagesGaoiran VS. Alcala, 444 SCRA 428 (2005)j0d3No ratings yet
- 3) Suzara vs. Benipayo. 176 SCRA 465Document17 pages3) Suzara vs. Benipayo. 176 SCRA 465Reihannah Paguital-MagnoNo ratings yet
- SBF Pale 1. Memorize Lawyer's Oath BELOWDocument3 pagesSBF Pale 1. Memorize Lawyer's Oath BELOWAnonymous ifiHUmx100% (1)
- Foitaf v. NorielDocument10 pagesFoitaf v. NorielDNAANo ratings yet
- Transformers 2 - Barops SolicitationDocument6 pagesTransformers 2 - Barops SolicitationrobjavierNo ratings yet
- CivRev2 - PNB Vs Manila Investment and Construction IncDocument6 pagesCivRev2 - PNB Vs Manila Investment and Construction IncAnonymous yisZNKXNo ratings yet
- Impact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsDocument4 pagesImpact of PNF-based Walking Exercise On A Ramp On Gait Performance of Stroke PatientsCristian Florin CrasmaruNo ratings yet
- Tong 2006Document7 pagesTong 2006Amanda BarrosNo ratings yet
- There Is No Superior Treatment in Improving Gait in Patients With Chronic StrokeDocument6 pagesThere Is No Superior Treatment in Improving Gait in Patients With Chronic Strokerc_delarosa5767No ratings yet
- Ergometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled TrialDocument6 pagesErgometer Cycling Improves The Ambulatory Function and Cardiovascular Fitness of Stroke Patients-A Randomized Controlled Trialayu lestariNo ratings yet
- Grammar activities and exercisesDocument29 pagesGrammar activities and exercisesElena NicolauNo ratings yet
- Commonlit Bloody KansasDocument8 pagesCommonlit Bloody Kansasapi-506044294No ratings yet
- GUIA REPASO 8° BÁSICO INGLÉS (Unidades 1-2)Document4 pagesGUIA REPASO 8° BÁSICO INGLÉS (Unidades 1-2)Anonymous lBA5lD100% (1)
- High Intermediate Analogies 9Document2 pagesHigh Intermediate Analogies 9Usman KhalidNo ratings yet
- Wave Optics Part-1Document14 pagesWave Optics Part-1Acoustic GuyNo ratings yet
- Dynamics of Bases F 00 BarkDocument476 pagesDynamics of Bases F 00 BarkMoaz MoazNo ratings yet
- New GK PDFDocument3 pagesNew GK PDFkbkwebsNo ratings yet
- Power of Positive Thinking EssayDocument7 pagesPower of Positive Thinking Essayafiboeolrhismk100% (2)
- Simon Baumberg - Prokaryotic Gene ExpressionDocument348 pagesSimon Baumberg - Prokaryotic Gene ExpressionBodhi Dharma0% (1)
- Reducing Healthcare Workers' InjuriesDocument24 pagesReducing Healthcare Workers' InjuriesAnaNo ratings yet
- Awareness Training On Filipino Sign Language (FSL) PDFDocument3 pagesAwareness Training On Filipino Sign Language (FSL) PDFEmerito PerezNo ratings yet
- How To Create A MetacogDocument6 pagesHow To Create A Metacogdocumentos lleserNo ratings yet
- HandoverDocument23 pagesHandoveryekoyesewNo ratings yet
- CPARDocument22 pagesCPARAngelo Christian MandarNo ratings yet
- Aviation Case StudyDocument6 pagesAviation Case Studynabil sayedNo ratings yet
- Novel anti-tuberculosis strategies and nanotechnology-based therapies exploredDocument16 pagesNovel anti-tuberculosis strategies and nanotechnology-based therapies exploredArshia NazirNo ratings yet
- Assignment Chemical Bonding JH Sir-4163 PDFDocument70 pagesAssignment Chemical Bonding JH Sir-4163 PDFAkhilesh AgrawalNo ratings yet
- TRU BRO 4pg-S120675R0 PDFDocument2 pagesTRU BRO 4pg-S120675R0 PDFtomNo ratings yet
- Pyrolysis: Mathematical Modeling of Hydrocarbon Pyrolysis ReactionsDocument8 pagesPyrolysis: Mathematical Modeling of Hydrocarbon Pyrolysis ReactionsBahar MeschiNo ratings yet
- Coek - Info Anesthesia and Analgesia in ReptilesDocument20 pagesCoek - Info Anesthesia and Analgesia in ReptilesVanessa AskjNo ratings yet
- Basic Statistical Tools for Data Analysis and Quality EvaluationDocument45 pagesBasic Statistical Tools for Data Analysis and Quality EvaluationfarjanaNo ratings yet
- Global Trustworthiness 2022 ReportDocument32 pagesGlobal Trustworthiness 2022 ReportCaroline PimentelNo ratings yet
- People v. De Joya dying declaration incompleteDocument1 pagePeople v. De Joya dying declaration incompletelividNo ratings yet
- United States v. Christopher King, 724 F.2d 253, 1st Cir. (1984)Document9 pagesUnited States v. Christopher King, 724 F.2d 253, 1st Cir. (1984)Scribd Government DocsNo ratings yet
- Newtons First LawDocument14 pagesNewtons First LawcaitlyntreacyNo ratings yet
- HexaflexDocument10 pagesHexaflexCharlie Williams100% (1)
- Corneal Ulcers: What Is The Cornea?Document1 pageCorneal Ulcers: What Is The Cornea?me2_howardNo ratings yet
- LAS IN ENTREPRENEURSHIP WEEK 4Document5 pagesLAS IN ENTREPRENEURSHIP WEEK 4IMELDA CORONACIONNo ratings yet
- 14 - Habeas Corpus PetitionDocument4 pages14 - Habeas Corpus PetitionJalaj AgarwalNo ratings yet
- Senator Frank R Lautenberg 003Document356 pagesSenator Frank R Lautenberg 003Joey WilliamsNo ratings yet