Professional Documents
Culture Documents
Acute Kidney Injury
Uploaded by
Rifhani Atthaya PutriOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Acute Kidney Injury
Uploaded by
Rifhani Atthaya PutriCopyright:
Available Formats
CASE REPORT
Acute Kidney Injury & Acute Glomerulonephritis
Compiled by :
Rifhani Atthaya Putri (120100124)
Yuli Bintang Theresia Sihotang (120100299)
Supervisor :
dr. Johannes Harlan Saing, M.Ked (Ped), Sp.A(K)
PEDIATRIC DEPARTEMENT
H. ADAM MALIK GENERAL HOSPITAL
FACULTY OF MEDICINE
UNIVERSITY OF SUMATERA UTARA
MEDAN
2016
ACKNOWLEDGEMENT
We are greatly indebt to the Almighty One for giving us blessing to finish
this case report, Acute Kidney Injury and Acute Glomerulonephritis. This case
report is requirement to complete the clinical assistance program in Department of
Child Health in Haji Adam Malik General Hospital, Medical Faculty of North
Sumatera University.
We are also indebt to our supervisor and adviser, dr. Johannes Harlan
Saing, M.Ked(Ped), Sp.A(K) for much spent time to give us guidance, comments,
and suggestions. We are grateful because without her, this case report wouldnt
have taken its present shape.
This case report has gone through series of developments and corrections.
There were critical but constructive and relevants suggestions from the reviewers.
Hopefully the content will be useful for everyone the future.
Medan, October 20th, 2016
Writer
s
CONTENTS
CONTENTS...................................................................................................
ii
CHAPTER 1 INTRODUCTION.................................................................
1.1 Acute Kidney Injury..................................................................................
1.2 Acute Glomerulonephritis.........................................................................
CHAPTER 2 LITERATURE REVIEW......................................................
2.1 Acute Kidney Injury................................................................................
2.1.1 Definition....................................................................................
2.1.2 Epidemiology..............................................................................
2.1.3 Etiology and Pathogenesis..........................................................
2.1.4 Clinical Manifestation................................................................
2.1.5 Diagnosis....................................................................................
2.1.6 Treatment....................................................................................
10
2.2 Acute Glomerulonephritis
2.2.1 Definition....................................................................................
15
2.2.2 Epidemiology.............................................................................
15
2.2.3 Etiology......................................................................................
15
2.2.3.1 Infectious ..........................................................................
16
2.2.3.2 Noninfectious....................................................................
16
2.2.4 Pathophysiology.........................................................................
17
2.2.5 Clinical Manifestation................................................................
18
2.2.6 Differential Diagnose.................................................................
19
2.2.7 Treatment....................................................................................
19
2.2.8 Complication..............................................................................
20
2.2.9 Prognosis....................................................................................
20
CHAPTER 3 CASE REPORT.....................................................................
21
CHAPTER 4 DISCUSSION.........................................................................
38
CHAPTER 5 SUMMARY ..........................................................................
43
REFERENCES..............................................................................................
44
CHAPTER 1
INTRODUCTION
1.1 Acute Kidney Injury
Acute kidney injury (AKI) is the sudden decline in renal function with
consequent loss of the kidney's ability to maintain homeostasis of body fluids.
Another source defines acute renal failure as a syndrome characterized by a
sudden decline in renal function that result of dumping the products of nitrogen
metabolites compounds such as urea and creatinine. According to Fine the criteria
for diagnosis of AKI is an increase in blood creatinine levels progressively 0.5 mg
/ dL per day. An increased level of blood urea is 10-20 mg / dL per day, except in
the event of circumstances hypercatabolism can reach 100 mg / dL per day.
Clinical manifestations of AKI may be oliguria or non oliguria. Nelson
defines oliguria as urine output <400 ml / m2 / day, oliguria. Alatas defines
oliguria in children is <240 ml / m 2 / day or 8-10 ml / kg / day 2. In neonates, the
criteria of oliguria is <1.0 ml / kg / hour, Ingelfinger impose limits <0.5 ml / kg /
day, while Gaudio and Siegel found each child can use the definition of <0,8cc /
kg / hour for all ages. In the non-oliguric AKI can be found diuresis > 1-2ml / kg /
h with rising levels of blood urea and creatinine. This condition is often found in
AKI by the use of nephrotoxic drugs including aminoglycosides.
In Department of Pediatric, Faculty of Medicine-RSCM Jakarta, from 38
patients with AKI were reported, 13 patients (34.2%) caused by intoxication, 11
(28%) by sepsis, 5 (13.2%) by severe gastroenteritis, 2 (5.2%) by shock and 2
(5.2%) by a severe bronchopneumonia. Acute glomerulonephritis only found in 3
children (7.9%). In two studies in western countries have reported the prevalence
of most cases of AKI in neonates due to perinatal asphyxia and shock. The
incidence of AKI in children with older age population is estimated at about
4/100000. In pre-school children, diarrhea followed by hemolytic-uremic
syndrome is the most common cause of intrinsic / renal AKI, accounting for 50%
of all cases in this group. Glomerulonephritis is the most common cause of AKI in
school age.
1.2 Acute Glomerulonephritis
GN represents 10-15% of glomerular diseases. Variable incidence has been
reported, in part because of the subclinical nature of the disease in more than half
the affected population. Despite sporadic outbreaks, the incidence of PSGN has
fallen over the past few decades. Factors responsible for this decline may include
better health care delivery and improved socioeconomic conditions.
Worldwide, IgA Nephropathy (Berger disease) is the most common cause
of GN. With some exceptions, the incidence of PSGN has fallen in most
developed
countries.
Japanese
researchers
reported
that
incidence
of
postinfectious GN in their country peaked in the 1990s, and that PSGN, which
accounted for almost all of the postinfectious GN cases in the 1970s, has
decreased to approximately 40-50% since the 1990s, while the proportion
of Staphylococcus aureus infectionrelated nephritis increased to 30%, and
hepatitis C virus infectionassociated GN also increased.
PSGN remains much more common in regions such as Africa, the
Caribbean, India, Pakistan, Malaysia, Papua New Guinea, and South America. In
Port Harcourt, Nigeria, the incidence of acute GN in children aged 3-16 years was
15.5 cases per year, with a male-to-female ratio of 1.1:1; the current incidence is
not much different. A study from a regional dialysis center in Ethiopia found that
acute GN was second only to hypovolemia as a cause of acute kidney injury that
required dialysis, accoujting for approximately 22% of cases. Geographic and
seasonal variations in the prevalence of PSGN are more marked for pharyngeally
associated GN than for cutaneously associated disease.
Postinfectious GN can occur at any age but usually develops in children.
Most cases occur in patients aged 5-15 years; only 10% occur in patients older
than 40 years. Outbreaks of PSGN are common in children aged 6-10 years. Acute
nephritis may occur at any age, including infancy. Acute GN predominantly
affects males (2:1 male-to-female ratio). Postinfectious GN has no predilection for
any racial or ethnic group. A higher incidence (related to poor hygiene) may be
observed in some socioeconomic groups.
CHAPTER 2
LITERATURE REVIEW
2.1 Acute Kidney Injury
2.1.1
Definition
Acute kidney injury (AKI), formerly called acute renal failure, is a clinical
syndrome in which a sudden deterioration in renal function results in the inability
of the kidneys to maintain fluid and electrolyte homeostasis. AKI occurs in 23%
of children admitted to pediatric tertiary care centers and in as many as 8% of
infants in the neonatal intensive care unit.
2.1.2 Epidemiology
No epidemiology studies using an established definition of AKI have been
conducted in pediatric patients. As described below, in pre-renal AKI the kidney is
intrinsically normal, and renal function promptly returns to normal with
restoration of adequate renal perfusion, while, in acute tubular necrosis, the
kidney has sustained intrinsic injury which requires repair and recovery before
renal function returns to normal. In a large study of adult patients, the incidence of
AKI was 209 per million population, and the most common cause of AKI was
pre-renal in 21% of patients and acute tubular necrosis in 45% of patients. Similar
epidemiologic studies have not been performed in pediatric patients, but
hypoxia/ischemia- and nephrotoxin-induced AKI have been shown to be
important causes of AKI in neonates, children and adolescents. In a study of
pediatric patients in a tertiary care center, 227 children received dialysis during an
8-year interval for an overall incidence of 0.8 per 100,000 total population.
In Department of Pediatric, Faculty of Medicine-RSCM Jakarta, from 38 patients
with AKI were reported, 13 patients (34.2%) caused by intoxication, 11 (28%) by
sepsis, 5 (13.2%) by severe gastroenteritis, 2 (5.2%) by shock and 2 (5.2%) by a
severe bronchopneumonia. Acute glomerulonephritis only found in 3 children
(7.9%). In two studies in western countries have reported the prevalence of most
cases of AKI in neonates due to perinatal asphyxia and shock. The incidence of
AKI in children with older age population is estimated at about 4/100000. In pre-
school children, diarrhea followed by hemolytic-uremic syndrome is the most
common cause of intrinsic / renal AKI, accounting for 50% of all cases in this
group. Glomerulonephritis is the most common cause of AKI in school age.
2.1.3 Etiology & Pathogenesis
AKI has been conventionally classified into three categories: prerenal,
intrinsic renal, and postrenal.
Prerenal AKI, also called prerenal azotemia, is characterized by
diminished effective circulating arterial volume, which leads to inadequate renal
perfusion and a decreased glomerular filtration rate (GFR). Evidence of kidney
damage is absent. Common causes of prerenal AKI include dehydration, sepsis,
hemorrhage, severe hypoalbuminemia, and cardiac failure. If the underlying cause
of the renal hypoperfusion is reversed promptly, renal function returns to normal.
If hypoperfusion is sustained, intrinsic renal parenchymal damage may develop.
Intrinsic renal AKI includes a variety of disorders characterized by renal
parenchymal damage, including sustained hypoperfusion/ischemia. Many forms
of glomerulonephritis, including postinfectious glomerulonephritis, lupus
nephritis,
Henoch-Schnlein
purpura
nephritis,
membranoproliferative
glomerulonephritis, and antiglomerular basement membrane nephritis, may
cause AKI.
Any form of glomerulonephritis in its most severe degree can present with
AKI and RPGN. The clinical features include hypertension, edema, hematuria that
is frequently gross, and a rapidly rising levels of blood urea nitrogen (BUN) and
creatinine. The characteristic pathological finding in RPGN is extensive crescent
formation. RPGN due to postinfectious glomerulonephritis typically does not lead
to CKD, while other glomerulonephritides, such as antineutrophil cytoplasmic
antibody (ANCA)-positive glomerulonephritis, Goodpastures syndrome, and
idiopathic RPGN, typically present with AKI and may quickly evolve into CKD,
with or without therapy. Serological tests including an antinuclear antibody
(ANA), ANCA, anti glomerular basement membrane (GBM) titers, and
complement studies are required to evaluate the etiology of the RPGN. Because
specific therapy will depend on the pathological findings, a biopsy should be
performed relatively quickly when a child presents with clinical characteristics
suggestive of RPGN.
Acute tubular necrosis (ATN) occurs most often in critically ill infants and
children who have been exposed to nephrotoxic and/or ischemic insults. The
typical pathologic process of ATN is tubular cell necrosis, although significant
histologic changes are not consistently seen in patients with clinical ATN. The
mechanisms of injury in ATN may include alterations in intrarenal
hemodynamics, tubular obstruction, and passive backleak of the glomerular
filtrate across injured tubular cells into the peritubular capillaries.
Tumor lysis syndrome is a specific form of AKI related to spontaneous or
chemotherapy-induced
cell
lysis
in
patients
with
lymphoproliferative
malignancies. This disorder is primarily caused by obstruction of the tubules by
uric acid crystals3.
Acute interstitial nephritis is an increasingly common cause of AKI and is
usually a result of a hypersensitivity reaction to a therapeutic agent or various
infectious agents.
Postrenal AKI includes a variety of disorders characterized by obstruction
of the urinary tract. In neonatal infants, congenital conditions such as posterior
urethral valves and bilateral ureteropelvic junction obstruction account for the
majority of cases of AKI. Other conditions such as urolithiasis, tumor (intraabdominal or within the urinary tract), hemorrhagic cystitis, and neurogenic
bladder may cause AKI in older children and adolescents. In a patient with two
functioning kidneys, obstruction must be bilateral to result in AKI. In general,
relief of the obstruction results in recovery of renal function except in patients
with associated renal dysplasia or prolonged urinary tract obstruction.
2.1.4
Clinical Manifestation
A carefully taken history is critical in defining the cause of AKI. An infant
with a 3-day history of vomiting and diarrhea most likely has prerenal AKI caused
by volume depletion. A 6-yr-old child with a recent pharyngitis who presents with
periorbital edema, hypertension, and gross hematuria most likely has intrinsic AKI
related to acute postinfectious glomerulonephritis. A critically ill child with a
history of protracted hypotension and exposure to nephrotoxic medications most
likely has ATN. A neonate with a history of hydronephrosis on prenatal ultrasound
and a palpable bladder most likely has congenital urinary tract obstruction,
perhaps related to posterior urethral valves.
The physical examination must be thorough, with careful attention to
volume status. Tachycardia, dry mucous membranes, and poor peripheral
perfusion suggest inadequate circulating volume and the possibility of prerenal
AKI. Peripheral edema, rales, and a cardiac gallop suggest volume overload and
the possibility of intrinsic AKI from glomerulonephritis or ATN. The presence of a
rash and arthritis may suggest systemic lupus erythematosus (SLE) or HenochSchnlein purpura nephritis. Palpable flank masses may suggest renal vein
thrombosis, tumors, cystic disease, or urinary tract obstruction.
2.1.5
Diagnosis
A detailed history and physical examination are invaluable for children
who develop AKI. Quantifying the urine output during the previous several days
may provide insight to the cause and severity of the episode of AKI and serves to
categorize the event as oliguric (defined as urine output <1 mL/kg/h) or
nonoliguric. Systematic evaluation of potential prerenal, intrinsic, and postrenal
causes is key to diagnosing the origin of AKI. Frequently, the history will provide
insight into causes or risk factors for prerenal AKI, including decreased
circulatory volume (gastroenteritis and hemorrhage), redistribution of circulatory
volume (edematous states, nephrotic syndrome, and sepsis), decreased cardiac
output (heart disease), or increased resistance to blood flow (abdominal
compartment syndrome and renal artery stenosis). In previously healthy children,
the history and physical examination may offer clues to the underlying intrinsic
renal origin, including volume depletion, recent viral illness or sore throat
(possibly consistent with acute glomerulonephritis), rashes, swollen joints
(suggesting systemic disorders such as lupus), hematuria, or medication
exposures.
When evaluating AKI, it is important to remember that an increase in
creatinine typically occurs up to 48 hours after renal injury and may reflect events
that occurred 2 to 3 days earlier. Therefore, it is important to review episodes of
hypotension, hypoxia, sepsis, surgery, contrast exposures, and drug exposures that
occur 48 to 72 hours before the episode of AKI becomes apparent.
If the cause of elevation in serum BUN and creatinine or oliguria is
unclear, entities that can be quickly addressed and corrected (eg, volume
depletion) should be considered first. Once normal renal perfusion is ensured and
no clinical evidence for de novo renal disease is present, a diagnosis of acute
tubular necrosis (vasomotor nephropathy, ischemic injury) may be entertained.
As part of the initial evaluation for AKI, patients should have the
following tests performed: basic electrolyte panel, serum creatinine measurement,
urinalysis, urine sodium measurement, urine urea measurement, urine creatine
measurement, urinalysis, and a renal ultrasound study. Urinalysis with
accompanying urine microscopy can be illuminating and point toward particular
diagnostic categories. Muddy granular casts on microscopy suggest ATN; red
blood cell casts suggest glomerulonephritis. A urinalysis positive for blood on
dipstick evaluation without evidence of red blood cells on microscopy should
raise
concerns
for
hemoglobinuria
(hemolysis)
or
myoglobinuria
(rhabdomyolysis).
The presence of hematuria, proteinuria, and/or red blood cell casts in the
right clinical scenario should raise concern for possible glomerulonephritis. In the
context of a recent upper respiratory tract infection, one should consider the
diagnosis of postinfectious glomerulonephritis (classically with pharyngitis 2-3
weeks earlier or skin infections 4-6 weeks earlier) and should evaluate serum
complements (low C3 and normal C4). In patients with a more recent upper
respiratory tract infection (2-3 days) with gross hematuria on urinalysis, one must
consider IgA nephropathy (normal complement levels). A urinalysis consistent
with glomerulonephritis in the context of the appropriate systemic symptoms (eg,
rash and arthritis) may point toward systemic lupus erythematosus (low C3 and
low C4) and may warrant further antibody testing (antinuclear and antidoublestranded DNA antibodies). In the setting of a classic clinical and laboratory
presentation of postinfectious glomerulonephritis, a renal biopsy is not warranted,
but to confirm the diagnosis and guide treatment of the remaining
glomerulonephritides, a biopsy is necessary. Each of the glomerulonephritides is
capable of causing rapidly progressive glomerulonephritis, which is defined by
rapidly increasing blood urea nitrogen and creatine levels. In this scenario, a renal
biopsy and treatment are immediately warranted because irreversible renal injury
may develop without prompt intervention.
The classic triad for allergic interstitial nephritis of fever, rash, and
eosinophilia is not often seen in the modern era and is observed in less than 15%
of patients. This is due to a change over time in the most common offending
agents. In patients with suspected interstitial nephritis, there is frequently bland
urine sediment that does not have red blood cell casts but may have white blood
cell casts present. The classic finding is urine eosinophils, although this is not
universal. There can be varying degrees of proteinuria; NSAID-associated
interstitial nephritis is capable of causing nephrotic range proteinuria. A renal
biopsy is necessary to confirm the diagnosis.
If a patient has a recent history of diarrheal illness, low platelet counts, and
hemolytic anemia with AKI, one should consider hemolytic uremic syndrome. In
the appropriate setting, a peripheral blood smear with schistocytes is confirmatory.
In recent years there has been an increase in the recognition of atypical hemolytic
uremic
syndrome
caused
by
nondiarrheal
infections
(eg, Streptococcus
pneumonia or human immunodeficiency virus) or genetic abnormalities in
complement regulatory components (eg, factor H or factor I); a high index of
suspicion is necessary, and specialty consultation is warranted.
Imaging plays a small role in the diagnosis of intrinsic renal disease.
Kidney size, measured by renal ultrasonography, can provide information about
the duration of the disease. Larger kidneys point toward an acute process that
involves active inflammation. Kidneys that are particularly small for age may
10
suggest a more chronic process. Often the kidneys will demonstrate increased
echogenicity in the setting of AKI, which is a nonspecific finding. A Doppler
evaluation of the renal vasculature is an important initial step if there are concerns
of renal artery stenosis, but if the result of the evaluation is negative and concern
of renal artery stenosis remains, further studies should be considered in
consultation with a pediatric nephrologist. Imaging by renal ultrasonography to
demonstrate hydronephrosis is the most important initial step in the diagnosis of
an obstructive process and may provide clues to the anatomical location of the
obstruction. For example, bilateral hydronephrosis suggests a more distal
obstruction. If an obstructive process is diagnosed, one should relieve the
obstruction immediately.
GFR (glomerular filtration rate) is equal to the total of the filtration rates
of the functioning nephrons in the kidney. GFR cannot be measured directly. In
clinical practice, serum levels of endogenous filtration markers, such as creatinine,
have traditionally been used to estimate GFR. To facilitate understanding of the
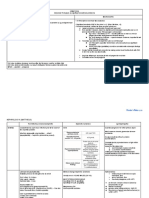
definition of AKI, a new classification system has created. RIFLE criteria (R risk
for renal dysfunction, I Injury to the kidney, F failure of kidney dysfunction, L
loss of kidney function, E end-stage renal disease) have been proposed as a
standard classification on acute kidney injury in adults and now has been adapted
for paediatric patients. RIFLE criteria is determined by the change of glomerular
filtration rate or urine output criteria.
Change in estimated Creatinine Clearance is calculated with:
Schwartz equation:
Length ( cm ) K (constant )
Serum Creatinine
The K(constant) are different between childrens ages
Neonates - 1 year old: k= 0,45
1 13 years old: k= 0,55
13 21 years old, boys k= 0,7; girls k= 0,57
11
Fig.2.1.5 Scheme for Defining Acute Kidney Injury4
2.1.6
Treatment
In infants and children with urinary tract obstruction, such as in a
newborn with suspected posterior urethral valves, a bladder catheter should be
placed immediately to ensure adequate drainage of the urinary tract. The
placement of a bladder catheter may also be considered in nonambulatory older
children and adolescents to accurately monitor urine output during AKI.
Determination of the volume status is of critical importance when initially
evaluating a patient with AKI. If there is no evidence of volume overload or
cardiac failure, intravascular volume should be expanded by intravenous
administration of isotonic saline, 20mL/kg over 30min. In the absence of blood
loss or hypoproteinemia, colloid-containing solutions are not required for volume
expansion.
Severe
hypovolemia
may
require
additional
fluid
boluses.
12
Determination of the central venous pressure may be helpful if adequacy of the
blood volume is in question. After volume resuscitation, hypovolemic patients
generally void within 2hr; failure to do so points toward the presence of intrinsic
or postrenal AKI.
Fluid replacement should be calculated based on the insensible water loss
(IWL) + the previous day's urine output plus the fluid out with vomit, stool,
nasogastric tube, etc. and corrected by a rise in temperature every 1 C as much
as 12% of body weight.
Diuretic therapy should be considered only after the adequacy of the
circulating blood volume has been established. Furosemide may be administered
as a single intravenous dose of 24mg/kg. To increase renal cortical blood flow,
many clinicians administer dopamine (23g/kg/min) in conjunction with diuretic
therapy, although there are no controlled data to support this practice.
If there is no response to a diuretic challenge, diuretics should be
discontinued and fluid restriction becomes essential. Patients with a relatively
normal intravascular volume should initially be limited to 400mL/m2/24hr
(insensible losses) plus an amount of fluid equal to the urine output for that day.
Extrarenal (blood, gastrointestinal tract) fluid losses should be replaced, milliliter
for milliliter, with appropriate fluids. On the other hand, markedly hypervolemic
patients may require further fluid restriction, omitting the replacement of
insensible fluid losses, urine output, and extrarenal losses to diminish the
expanded intravascular volume. In general, glucose-containing solutions (10
30%) without electrolytes are used as maintenance fluids and the composition of
the fluid modified according to the state of electrolyte balance. Fluid intake, urine
and stool output, body weight, and serum chemistries should be monitored on a
daily basis1. Converting oliguric to non-oliguric renal failure may help with fluid
and electrolyte management, but does not seem to affect eventual need for dialysis
or overall mortality, and should not delay the start of renal replacement therapy
when otherwise indicated.
In AKI, rapid development of hyperkalemia(serum potassium level > 6
mEq/L) may lead to cardiac arrhythmia, cardiac arrest, and death. Procedures to
13
deplete body potassium should be initiated when the serum potassium value rises
to 6.0mEq/L. Exogenous sources of potassium (dietary, intravenous fluids, total
parenteral nutrition) should be eliminated.
Acidosis is common in AKI as a result of retention of hydrogen ions,
phosphate, and sulfate. If acidosis is severe (arterial pH < 7.15; serum bicarbonate
< 8mEq/L) or contributes to hyperkalemia, treatment is required. The acidosis
should be corrected partially by the intravenous route, generally giving enough
bicarbonate to raise the arterial pH to 7.20 (which approximates a serum
bicarbonate level of 12mEq/L). The remainder of the correction may be
accomplished by oral administration of sodium bicarbonate after normalization of
the serum calcium and phosphorus levels. Sodium bicarbonate can be given based
on the blood gases analysis (BE weight 0,3 mEq). Correction of metabolic
acidosis with intravenous bicarbonate may precipitate tetany in patients with renal
failure as rapid correction of acidosis reduces the ionized calcium concentration 2.
Sodium bicarbonate administration usually, although not always corrects the
acidosis, rising serum bicarbonate concentration, serum pH, and the partial
pressure of carbon dioxide, but evidence for clinical benefit derived from this
effect is not conclusive.
Hypocalcemia is primarily treated by lowering the serum phosphorus
level. Calcium should not be given intravenously, except in cases of tetany (Ca
Gluconas 10% 0,5 ml/kgBW) to avoid deposition of calcium salts into tissues2.
Patients should be instructed to follow a low phosphorus diet, and phosphate
binders should be given by mouth to bind any ingested phosphate and increase
gastrointestinal phosphate excretion. The total daily dose should be gradually
increased until the serum phosphorus level falls to normal.
Hyponatremia is most commonly a dilutional disturbance, which must be
corrected by fluid restriction rather than sodium chloride administration 1.
Administration of hypertonic 3% saline (0,5 mg/ml) should be limited to those
patients with symptomatic hyponatremia (seizures, lethargy) or those with serum
sodium level less than 120mEq/L. Acute correction of the serum sodium to 125
14
mEq/L (mmol/L) should be accomplished using the following formula: mEq NaCl
required = 0,6 x weight (kg) x (125 serum sodium).
Nutrition is of critical importance in children who develop ARF. In most
cases, sodium, potassium, and phosphorus should be restricted. Protein intake
should be restricted moderately while maximizing caloric intake to minimize the
accumulation of nitrogenous wastes. In critically ill patients with ARF, parenteral
hyperalimentation with essential amino acids should be considered.
The patients caloric intake calculations are based on caloric expenditure is
as follows:
Figure 2.1.6 Caloric and water needs per unit of body weight6
Protein needs: 2 g / kg BW / day2.
Dialysis. Indications for hemodialysis / peritoneal dialysis in AKI include
the following2:
Volume overload with evidence of hypertension and/or pulmonary edema
refractory to diuretic therapy
Persistent hyperkalemia > 7,5 mEq/L
Severe metabolic acidosis unresponsive to medical management
Neurologic symptoms (altered mental status, seizures)
Blood urea nitrogen greater than 100150mg/dL (or lower if rapidly
rising)
Serum ureum level > 200 mg/dl
Continuous renal replacement therapy(CRRT) is useful in patients with
unstable hemodynamic status, concomitant sepsis, or multiorgan failure in the
intensive care setting. CRRT is an extracorporeal therapy in which fluid,
15
electrolytes, and small-and medium-sized solutes are continuously removed from
the blood (24hr/day) using a specialized pump-driven machine. Usually, a doublelumen catheter is placed into the subclavian, internal jugular, or femoral vein. The
patient is then connected to the pump-driven CRRT circuit, which continuously
passes the patient's blood across a highly permeable filter.
Infectious complications are often a cause of death in AKI. Urine catheter,
if no longer needed, should be removed because it can cause nosocomial
infections. Antibiotic prophylaxis is not recommended because it can cause
resistant strains of germs and candidiasis. But when an infection occurs, it must be
eradicated with adequate antibiotics. The use of nephrotoxic drugs be avoided
whenever possible.
2.1.7
Prognosis
The mortality rate in children with AKI is variable and depends entirely
on the nature of the underlying disease process rather than on the renal failure
itself. In general, children with AKI caused by a renal-limited condition such as
postinfectious glomerulonephritis have a very low mortality rate (<1%); those
with AKI related to multiorgan failure have a very high mortality rate (>90%).
Historically, nonoliguric renal failure has been assumed to have a better outcome
than oliguric renal failure9.
The prognosis for recovery of renal function depends on the disorder
that precipitated the AKI. In general, recovery of function is likely after AKI
resulting from prerenal causes, HUS, ATN, acute interstitial nephritis, or tumor
lysis syndrome. On the other hand, recovery of renal function is unusual when
AKI results from most types of rapidly progressive glomerulonephritis, bilateral
renal vein thrombosis, or bilateral cortical necrosis3.
Medical management may be necessary for a prolonged period of time
to treat sequelae of AKI, including chronic renal insufficiency, hypertension, renal
tubular acidosis, and urinary concentrating defect1.
16
2.2 Acute Glomerulonephritis
2.2.1
Definition
Acute glomerulonephritis (GN) comprises a specific set of renal diseases
in which an immunologic mechanism triggers inflammation and proliferation of
glomerular tissue that can result in damage to the basement membrane,
mesangium, or capillary endothelium. Acute nephritic syndrome is the most
serious and potentially devastating form of the various renal syndromes.
Acute
GN
is
defined
as
glomerular
inflamation
which
histopathologically show proliferation and inflammation of glomeruli cells;
started by group A -hemolytic streptococci infection. Usually manifest as acute
nephritic syndrome like the sudden onset of hematuria, proteinuria, and red blood
cell (RBC) casts in the urine. Acute nephritic syndrome is a clinical symptoms
like proteinuria, hematuria, azotemia, red blood cast, oliguria, and hypertension
(PHAROH) which occurred suddenly. This clinical picture is often accompanied
by hypertension, edema, azotemia (ie, decreased glomerular filtration rate [GFR]),
and renal salt and water retention. Acute GN can be due to a primary renal disease
or to a systemic disease. Most original research focuses on acute PSGN.
2.2.2
Epidemiology
Postinfectious GN can occur at any age but usually develops in children.
Most cases occur in patients aged 5-15 years, only 10% occur in patients older
than 40 years. Outbreaks of PSGN are common in children aged 6-10 years. Acute
nephritis may occur at any age, including infancy. Acute GN predominantly
affects males (2:1 male-to-female ratio). Postinfectious GN has no predilection for
any racial or ethnic group. A higher incidence (related to poor hygiene) may be
observed in some socioeconomic groups.
17
2.2.3
Etiology
The causal factors that underlie acute GN can be broadly divided into
infectious and noninfectious groups.
2.2.3.1 Infectious factor
The most common infectious cause of acute GN is infection
by Streptococcus species (i.e., group A, beta-hemolytic). Two types have been
described, involving different serotypes :
Serotype 12 - Poststreptococcal nephritis due to an upper respiratory infection.
Serotype 49 - Poststreptococcal nephritis due to a skin infection
PSGN usually develops 1-3 weeks after acute infection with specific
nephritogenic strains of group A beta-hemolytic Streptococcus. The incidence of
GN is approximately 5-10% in persons with pharyngitis and 25% in those with
skin infections. Nonstreptococcal postinfectious GN may also result from
infection by other bacteria, viruses, parasites, or fungi. Bacteria besides group A
Streptococci that can cause acute GN include Diplococci, Staphylococci, and
mycobacteria. Salmonella
typhosa, Brucellasuis, Treponema
pallidum,
Corynebacterium bovis, and Actinobacilli have also been identified.
2.2.3.2 Noninfectious factor
Noninfectious causes of acute GN may be divided into primary renal
diseases and systemic diseases. Multisystem systemic diseases that can cause
acute GN include the following:
-
Vasculitis (e.g., granulomatosis with polyangiitis [Wegener granulomatosis]):
This causes glomerulonephritis that combines upper and lower granulomatous
nephritides.
Collagen-vascular diseases (e.g., systemic lupus erythematosus [SLE]) : This
causes glomerulonephritis through renal deposition of immune complexes.
Hypersensitivity vasculitis : This encompasses a heterogeneous group of
disorders featuring small vessel and skin disease.
18
Polyarthritis nodosa : This causes nephritis from a vasculitis involving the
renal arteries.
Henoch-Schnlein purpura : This causes a generalized vasculitis resulting in
glomerulonephritis.
Goodpasture syndrome : This causes circulating antibodies to type IV collagen
and often results in a rapidly progressive oliguric renal failure (weeks to
months).
Primary renal diseases that can cause acute GN include the following:
1. Membranoproliferative glomerulonephritis (MPGN) : This is due to the
expansion and proliferation of mesangial cells as a consequence of the
deposition of complements. Type I refers to the granular deposition of C3,
type II refers to an irregular process.
2. Berger disease (IgG-immunoglobulin A [IgA] nephropathy) : This causes GN
as a result of diffuse mesangial deposition of IgA and IgG.
3. Pure mesangial proliferative GN
4. Idiopathic rapidly progressive glomerulonephritis : This form of GN is
characterized by the presence of glomerular crescents. Three types have been
distinguished : Type I is an antiglomerular basement membrane disease, type
II is mediated by immune complexes, and type III is identified by
antineutrophil cytoplasmic antibody (ANCA).
2.2.4
Pathophysiology
Glomerular lesions in acute GN are the result of glomerular deposition or
in situ formation of immune complexes. On gross appearance, the kidneys may be
enlarged up to 50%. Histopathologic changes include swelling of the glomerular
tufts and infiltration with polymorphonucleocytes. Immunofluorescence reveals
deposition of immunoglobulins and complement.
Except in PSGN, the exact triggers for the formation of the immune
complexes are unclear. In PSGN, involvement of derivatives of streptococcal
proteins has been reported. A streptococcal neuraminidase may alter host
immunoglobulin G (IgG). IgG combines with host antibodies. IgG/anti-IgG
19
immune complexes are formed and then collect in the glomeruli. In addition,
elevations of antibody titers to other antigens, such as antistreptolysin O or
antihyaluronidase, DNAase-B, and streptokinase, provide evidence of a recent
streptococcal infection.
Structural and functional changes
Acute GN involves both structural changes and functional changes.
Structurally, cellular proliferation leads to an increase in the number of cells in the
glomerular tuft because of the proliferation of endothelial, mesangial, and
epithelial cells. The proliferation may be endocapillary (i.e., within the confines of
the glomerular capillary tufts) or extracapillary (i.e., in the Bowman space
involving the epithelial cells). In extracapillary proliferation, proliferation of
parietal epithelial cells leads to the formation of crescents, a feature characteristic
of certain forms of rapidly progressive GN. Leukocyte proliferation is indicated
by the presence of neutrophils and monocytes within the glomerular capillary
lumen and often accompanies cellular proliferation. Glomerular basement
membrane thickening appears as thickening of capillary walls on light
microscopy. On electron microscopy, this may appear as the result of thickening
of basement membrane proper (e.g., diabetes) or deposition of electron-dense
material, either on the endothelial or epithelial side of the basement membrane.
Electron-dense deposits can be subendothelial, subepithelial, intramembranous, or
mesangial, and they correspond to an area of immune complex deposition.
Hyalinization or sclerosis indicates irreversible injury. These structural changes
can be focal, diffuse or segmental, or global. Functional changes include
proteinuria, hematuria, reduction in GFR (i.e., oligoanuria), and active urine
sediment with RBCs and RBC casts. The decreased GFR and distal nephron salt
and water retention result in expansion of intravascular volume, edema, and,
frequently, systemic hypertension.
2.2.5
Clinical Manifestation
Patients often have a normal physical examination and blood pressure.
Most frequently, however, patients present with a combination of edema,
20
hypertension, and oliguria. Some patient may present the following signs of fluid
overload :
1. Periorbital and/or pedal edema
2. Edema and hypertension due to fluid overload (in 75% of patients)
3. Crackles (i.e., if pulmonary edema)
4. Elevated jugular venous pressure
5. Ascites and pleural effusion (possible)
Some patient may present with other sign, for example :
1. Rash (as with vasculitis, Henoch-Schnlein purpura, or lupus nephritis)
2. Renal angle (i.e., costovertebral) fullness or tenderness, joint swelling, or
tenderness
3. Hematuria, either macroscopic or microscopic
4. Abnormal neurologic examination or altered level of consciousness
2.2.6
Differential Diagnoses
Acute GN must be differentiated from the following conditions :
1. Acute Kidney Injury
2. Nephrotic Syndrome
3. Chronic Kidney Failure
4. Renal Tumor
5. Chronic GN with an acute exacerbation
6. Familial nephritis
2.2.7
Treatment
Treatment of glomerulonephritis depend on whether you have an acute or
chronic form of the disease, the underlying cause, and the type and severity of
your signs and symptoms. Some cases of acute glomerulonephritis, especially
those that follow a streptococcus infection, tend to improve on their own and often
require no specific treatment. In general, the goal of treatment is to protect your
kidneys from further damage.
21
Keeping blood pressure under control is key to protecting kidneys. To control
high blood pressure and slow the decline in kidney function, doctor may prescribe
one of several medications, including :
-
Diuretics
Angiotensin-converting enzyme (ACE) inhibitors
Angiotensin II receptor blockers
If there's an underlying cause for kidney inflammation, doctor may
prescribe other drugs to treat the underlying problem, in addition to
treatment to control any hypertension :
Streptococcus or other bacterial infection. Treatment usually focuses on
easing your signs and symptoms. Your doctor also may prescribe an
appropriate antibiotic.
Lupus or vasculitis. Doctors often prescribe corticosteroids and immunesuppressing drugs to control inflammation.
IgA nephropathy. In some cases, both fish oil supplements and certain
immune-suppressing drugs can successfully treat certain people with IgA
nephropathy. Researchers continue to investigate fish oil supplements for IgA
nephropathy.
Goodpasture's syndrome. Plasmapheresis is sometimes used to treat people
with Goodpasture's syndrome. Plasmapheresis is a mechanical process that
removes antibodies from your blood by taking some of your plasma out of
your blood and replacing it with other fluid or donated plasma.
2.2.
Complication
1. Hypertension Encephalopathy
2. Acute Kidney Injury
3. Lung Oedema
4. Posterior Leukoencephalopathy Syndrome
22
2.2.9
Prognosis
Most epidemic cases follow a course ending in complete patient recovery
(as many as 100%). The mortality of acute GN in the most commonly affected age
group, pediatric patients, has been reported at 0-7%. Sporadic cases of acute
nephritis often progress to a chronic form. This progression occurs in as many as
30% of adult patients and 10% of pediatric patients. GN is the most common
cause of chronic renal failure (25%).
CHAPTER 3
CASE REPORT
3.1.
Case Objective
The objective of this paper is to report a case of a 10 years 8 months 13
days old boy with a diagnosis of Acute Kidney Injury Stadium Injury e.c Acute
Glomerulonephritis.
3.2.
Case
RS, boy aged 10 years 8 months 13 days, came to Haji Adam Malik
Hospital on September 26, 2016 with chief complaints of red coloured urine.
3.3.
History of Disease
RS, boy aged 10 years 8 months 13 days, came to Haji Adam Malik
Hospital on September 26, 2016 with a chief complaint of red coloured urine
since 10 days ago. He has pain during urination since 10 days ago, two times
per day with volume 50 cc / 24 hours. Its color is meat colour wash. Pain flank
was not found.
He experienced facial and foot edema since 10 days ago. Facial edema is
first occured when RS woke up in the morning and is mainly located in superior
palpebrae. Fever was found since 14 days ago. Body temperature is not too
23
high. The fever pattern can went up and down. Fever can be decreased with feverreducing drug. When RS admitted to HAM hospital fever was not found.
Shivering was not found. Seizure and history of being seizure before wasnt
found.
Cough and sore throat were experienced for this 1 month. It was a dry
cough. Contact with an adult person with coughing disease wasnt found. He felt
nausea and vomitting since 2 days ago, five times per day with average volume
glass of mineral water each vomit. The content of the vomit is the patients diet.
The defecation is normal.
He was referred to Haji Adam Malik Hospital from Harapan Pematang
Siantar Hospital with Acute Glomerulonephritis.
History of Medication
History of family
History of parents medication
History of Pregnancy
History of Birth
: Amoxicillin, Furosemide, and Captopril
: None
: None
: None
: Birth was assisted by doctor. The patient
was born pervaginam and cried loudly
immediately after birth. Body
weight at
birth was 3000 grams, body length at birth
was unclear. Cyanosis(-), Jaundice (-)
History Of feeding
History of immunization
: a. Breastfeeding : exclusive, 6 months
b. Formula milk : 7 months
c. Milk porridge: 8 months
d. Rice porridge : 9 months
e. Adult food : 12 months
: Immunization was complete
History of growth and development: Not clear. Patients mom didnt remember
about
the
development.
Physical Examination:
Present status:
patients
growth
and
24
Sensorium
: Compos Mentis
Blood Pressure
: 140/90 mmHg
Heart Rate
: 90 x/minute
Respiratory Rate
: 22 x/minute
Body temperature
: 36,9 C
Body Weight
: 28 kg
Body Length
: 134 cm
BW/A
: 77 %
BL/A
: 92 %
BW/BL
: 100 %
GCS : 15 (E4M6V5)
Cyanosis (-), Anemic (-), Icteric (-), Dyspnea (-), Edema (+)
Localized status
Head :
Face
Eye
Ear
Nose
Mouth
Neck
Thorax
Abdomen
Extremities
Anogenital
Differential diagnosis
: Edema (+)
: Light reflex (+/+), isochoric pupil, pale inferior
palpebral conjunctiva (+/+), palpebra oedema (+/+)
: Both ear lobe in normal morphologic.
: Septum deviation (-), normal morphologic.
: Mouth mucosal pale (-)
: Lymph node enlargement (-)
: Symmetrical fusiform, retraction (-)
HR: 90bpm, regular, murmur (-/-)
RR: 22 per minute, regular, ronchi (-/-)
: Soepel, shifting dullness (-), normal peristaltic,
liver and spleen unpalpable
: Pulse 90 bpm, regular, adequate p/v, felt warm
CRT<3, pale plantar palmar (+)
: Male, enlargement scrotum (-)
: Acute Kidney Injury Stadium Injury
Acute Glomerulonephritis
IgA Nephropathy
Nephrotic Syndrome
Working diagnosis
: Acute Kidney Injury Stadium Injury e.c. Acute
Glomerulonephritis + Metabolic Acidosis
25
Laboratory finding:
Complete Blood Analysis (September 27th 2016)
Test
Hemoglobin
Erythrocyte
Leucocyte
Thrombocyte
Hematocrite
Eosinophil
Basophil
Neutrophil
Lymphocyte
Monocyte
Neutrophil absolute
Lymphocyte absolute
Monocyte absolute
Eosinophil absolute
Basophil absolute
MCV
MCH
MCHC
RDW
MPV
PDW
PCT
Result
8.2
3.05
15.310
318
24
0.70
0.30
80.70
12.70
5.60
12.35
1.95
0.86
0.10
0.05
80
26.9
33.7
12.4
9.4
9.0
0.300
Unit
g/dL
106/L
/L
103/L
%
%
%
%
%
%
103/L
103/L
103/L
103/L
103/L
fL
pg
g/dL
%
fL
%
%
References
13 18
4,50 6,50
4.000 11.000
150 450
39 54
1,00 3,00
0,00 1,00
50,00 70,00
20,00 40,00
2,00 8,00
2,4 7,3
1,7 5,1
0,2 0,6
0,10 0,30
0 0,1
81 99
27 31
31 37
11,5 14,5
6,5 9,5
10,0 18,0
0,100 0,500
26
Clinical Chemistry
Blood Gas Analysis
pH
pCO2
pO2
Bicarbonat (HCO3)
Total CO2
BE
Saturation O2
7.270
17.0
174.0
7.8
8.3
-16.8
99.0
mmHg
mmHg
mmol/L
mmol/L
mmol/L
%
7,35 7,45
38 42
85 100
22 26
19 25
(-2) (+2)
95 100
2.5
g/dL
3,5 5,0
83
mg/dL
<200
Liver Function
Albumin
Carbohydrate Metabolism
Blood Glucosa
Renal Function
Blood Urea Nitrogen
Ureum
Creatinin
48
103
1.39
mg/dL
mg/dL
mg/dL
9-21
19-44
0.7-1.3
132
3.5
99
7.20
mEq/L
mEq/L
mEq/L
mg/dL
135-155
3.6-5.5
96-106
8.4-10.2
Electrolyte
Natrium
Kalium
Clorida
Kalsium
27
Urinalysis
Complete Urine
Color
Glucose
Bilirubin
Keton
Berat Jenis
pH
Protein
Urobilinogen
Nitrit
Leucocyte
Blood
Yellow cloudy
Negative
Negative
Negative
1.010
5.0
+
Positive
Positive
Positive
Positive
Yellow
Negative
Negative
Negative
1.005-1.030
5-8
Negative
Negative
Negative
Urine Sedimen
Erytrocyte
Leucocyte
Epithelial
Casts
Crystal
Therapy
50 60
20 30
01
Negative
Uric Acid 2-4
:
Non Pharmacology :
Bed rest
IVFD D5% 4cc/hours (micro)
Pharmacology :
Inj. Ondansetron 3 mg/ 12 hours/ IV
Bicnat 1 1 1
Furosemid 2 x 20 mg
Valsartan 1 x 20 mg
Calnix syr 3 x Cth I
FOLLOW UP
S
September, 26th 2016
Red colour urine (+), vomit (+)
LPB
LPB
LPB
LPB
LPB
<3
<6
Negative
28
Sensorium
CM, T: 36.6C
Head
Face: Oedema (+).
Eyes:
Isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
+), oedema superior palpebra (+/+). E/N/M : N
Lymph node enlargement (-)
Neck
SF, retraction (-). Heart rate 90 beats/min, regular,
Thorax
murmur (-). Respiratory rate 22 breaths/min, regular,
ronchi (-/-)
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
Abdomen
and spleen undetermined, shifting dullness (-)
Pulse 90 times/min, regular, blood pressure 140/90
Extremities
mmHg, adequate pressure and volume, warm, CRT <
3. Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis +
Metabolic Acidosis
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Ondansetron 3 mg/ 12 hours/ IV
Bicnat 1 1 1
Furosemid 2 x 20 mg
Valsartan 1 x 20 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1450 ml (N: 672 1008 ml)
Creatinine Clearance :
Schwartz equation:
134 0,55
=53,02
(N = 96,5 s/d 136,9)
1,39
eCr < 50% (Stadium Injury)
R/ Dipstick Urine/6 hours
29
Urinalysis, Urine Culture
C3 Complement, ASTO, CRP
Throat swab
S
O
September, 27th 2016
Red colour urine (+), vomit (+)
Sensorium
CM, T: 36.9C
Head
Face: Oedema (+).
Eyes:
Isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
+), oedema superior palpebra (+/+). E/N/M are
normal.
Neck
Lymph node enlargement (-)
Thorax
SF, retraction (-). Heart rate 90 beats/min, regular,
murmur (-). Respiratory rate 22 breaths/min, regular,
ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
and spleen undetermined, shifting dullness (-)
Extremities
Pulse 90 times/min, regular, blood pressure 100/80
mmHg, adequate pressure and volume, warm, CRT <
3. Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis +
Metabolic Acidosis
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Ondansetron 3 mg/ 12 hours/ IV
Bicnat 1 1 1
Furosemid 2 x 20 mg
Valsartan 1 x 20 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1300 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
30
S
O
/ + / 0,2 / +++ /6,0/ +++ /1.015/ - / + / September, 28th 2016
Red colour urine (+), vomit (-)
Sensorium
CM, T: 36.5C
Head
Face: Oedema (+).
Eyes:
Isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
+), oedema superior palpebra (+/+).
Neck
E/N/M are normal.
Thorax
Lymph node enlargement (-)
SF, retraction (-). Heart rate 90 beats/min, regular,
murmur (-). Respiratory rate 24 breaths/min, regular,
ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
and spleen undetermined, shifting dullness (-)
Extremities
Pulse 90 times/min, regular, blood pressure 100/80
mmHg, adequate pressure and volume, warm, CRT <
3. Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis +
Acidosis Metabolic
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Ondansetron 3 mg/ 12 hours/ IV
Bicnat 1 1 1
Furosemid 2 x 20 mg
Valsartan 1 x 20 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
Advice from Supervisor : Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV
Eas primer 10 cc/12 hours finish in 1 hour
Captopril 2 x 12,5 mg
Bicnat 2 2 2
31
Acidosis metabolic correction :
1
( 0,6 x 28 x 16,8 ) =28,56 29 meq
4
With meylon 29 meq in D5% 145 cc finish in 4 hours
UOP 24 hours : 1400 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
- / + / 0,2 / + /6,0/ +++ /1.010/ - / - / Laboratory Result :
-
ASTO
: <200
CRP
: 1.4 mg/dL
S
O
C3 Complement : 36 mg/dL
September, 29th 2016
Red colour urine (+)
Sensorium
CM, T: 36.6C
Head
Face: Oedema (+).
Eyes:
Isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
+), oedema superior palpebra (+/+). E/N/M are
normal.
Neck
Lymph node enlargement (-)
Thorax
SF, retraction (-). Heart rate 88 beats/min, regular,
murmur (-). Respiratory rate 20 breaths/min, regular,
ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
and spleen undetermined, shifting dullness (-)
Extremities
Pulse 88 times/min, regular, blood pressure 100/80
mmHg, adequate pressure and volume, warm, CRT <
3. Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis +
Acidosis Metabolic (Post-Correction Meylon)
Bed rest
IVFD D5% 4cc/hours (micro)
32
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-1)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 2 2 2
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
Advice from Supervisor : Consul to urologic surgery Susp. VUR
KSR 3 x 1 tab
Bicnat 1 1 1
Drink 200 cc/6 hours
UOP 24 hours : 1150 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
+ / + / 0,2 / /5,0/ ++ /1.015/ - / - / Blood Gas Analysis
pH / PCO2 / PO2 / HCO3 / TCO2 / BE / SaO2
7,566 / 20,2 / 173,5 / 17,9 / 18,6 / -1,6 / 99%
Electrolyte
Ca / Na/ K / Cl = 7 / 124 / 2,8 / 93
R / Hyponatremia correction : (135 124) x 0,6 x 28 = 184,8 meq
maintenance 56 meq, TOT: 240,8 meq
S
O
with NaCl 0,9% 32 gtt/i (micro) for 48 hours
September, 30th 2016
Red colour urine (+)
Sensorium
CM, T: 37.3C
Head
Face: Oedema (+).
Eyes:
Isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
33
+), oedema superior palpebra (+/+). E/N/M are
Neck
normal.
Lymph node enlargement (-)
Thorax
SF, retraction (-). Heart rate 108 beats/min, regular,
murmur (-). Respiratory rate 20 breaths/min, regular,
ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
and spleen undetermined, shifting dullness (-)
Extremities
Pulse 108 times/min, regular, blood pressure 100/80
mmHg, adequate pressure and volume, warm, CRT <
A
P
3. Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-2)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 1 1 1
KSR 3 x 1 tab
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1100 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
S
O
- / + / 0,2 / ++ /6,0/ ++ /1.010/ - / + / October, 1st 2016
Red colour urine (+)
Sensorium
CM, T: 37.3C
Head
Face: Oedema (+).
Eyes: Isochoric pupil, pale inferior palpebral conjunctiva
(+/+), icteric sclera (-/-), light reflexes (+/+), oedema
superior palpebra (+/+). E/N/M are normal.
Neck
Lymph node enlargement (-)
34
Thorax
SF, retraction (-). Heart rate 108 beats/min, regular, murmur
(-). Respiratory rate 20 breaths/min, regular, ronchi (-/-)
Symmetric, soepel, peristaltic (+) normal. Kidney, liver and
Abdomen
spleen undetermined, shifting dullness (-)
Pulse 108 times/min, regular, blood pressure 100/80
Extremities
A
P
mmHg, adequate pressure and volume, warm, CRT < 3.
Pale plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-3)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 1 1 1
KSR 3 x 1 tab
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1050 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
S
O
- / + / 0,2 / ++ /6,0/ ++ /1.010/ - / + / October, 2nd 2016
Red colour urine (+), fever (+), vomit (+)
Sensorium
CM, T: 38.4C
Head
Face: Oedema (+).
Eyes:
isochoric
pupil,
pale
inferior
palpebral
conjunctiva (+/+), icteric sclera (-/-), light reflexes (+/
+), oedema superior palpebra (+/+).
Neck
E/N/M are normal.
Thorax
Lymph node enlargement (-)
SF, retraction (-). Heart rate 100 beats/min, regular,
murmur (-). Respiratory rate 20 breaths/min, regular,
ronchi (-/-)
35
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver
and spleen undetermined, shifting dullness (-)
Extremities
Pulse 100 times/min, regular, blood pressure 100/80
mmHg, adequate pressure and volume, warm, CRT < 3.
A
P
Pale plantar palmar (+)
Acute Glomerulonephritis
Bed rest
IVFD D5% 4cc/hours (micro)
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-4)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 1 1 1
KSR 3 x 1 tab
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1200 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
S
O
/ - / 0,2 / + /6,0/ +++ /1.015/ - / - / October, 3rd 2016
Red colour urine (+), fever (+), vomit (-)
Sensorium
CM, T: 38.3C
Head
Face: Oedema (+).
Eyes: isochoric pupil, pale inferior palpebral conjunctiva
(+/+), icteric sclera (-/-), light reflexes (+/+), oedema
superior palpebra (+/+).
Neck
E/N/M are normal.
Thorax
Lymph node enlargement (-)
SF, retraction (-). Heart rate 96 beats/min, regular, murmur
(-). Respiratory rate 20 breaths/min, regular, ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver and
spleen undetermined, shifting dullness (-)
Extremities
Pulse 96 times/min, regular, blood pressure 100/60 mmHg,
36
adequate pressure and volume, warm, CRT < 3. Pale
A
P
plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis
Bed rest
Threeway
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-4)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 1 1 1
KSR 3 x 1 tab
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1200 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
S
O
- / + / 0,2 / /5,0/ ++ /1.010/ - / - / October, 4th 2016
Red colour urine (+), fever (+), vomit (-)
Sensorium
CM, T: 38.2C
Head
Face: Oedema (+).
Eyes: isochoric pupil, pale inferior palpebral conjunctiva
(+/+), icteric sclera (-/-), light reflexes (+/+), oedema
superior palpebra (+/+).
Neck
E/N/M are normal.
Thorax
Lymph node enlargement (-)
SF, retraction (-). Heart rate 88 beats/min, regular, murmur
(-). Respiratory rate 20 breaths/min, regular, ronchi (-/-)
Abdomen
Symmetric, soepel, peristaltic (+) normal. Kidney, liver and
spleen undetermined, shifting dullness (-)
Extremities
Pulse 88 times/min, regular, blood pressure 100/60 mmHg,
adequate pressure and volume, warm, CRT < 3. Pale
A
P
plantar palmar (+)
Acute Kidney Injury Std. Injury e.c. Acute Glomerulonephritis
Bed rest
37
Threeway
Inj. Paracetamol 300 mg/8 hours/IV
Inj. Ceftriaxone 1 gr/12 hours/IV (D-6)
Eas primer 10 cc/12 hours finish in 1 hour
Bicnat 1 1 1
KSR 3 x 1 tab
Captopril 2 x 12,5 mg
Calnix syr 3 x Cth I
Adult food low salt diet, 1660 kcal with 56 gr protein
UOP 24 hours : 1300 ml (N: 672 1008 ml)
Urine Dipstick
LEU/NIT/URO/PRO/PH/BLO/SG /KET/BIL/GLU
- / + / 0,2 / /5,0/ ++ /1.010/ - / - / R/ Blood culture
October, 4th 2016: The patient was discharged.
38
CHAPTER 4
CASE DISCUSSION
THEORY
CASE
Definition : Acute GN is defined as the Hematuria : +++
Proteinuria : +
sudden onset of hematuria, proteinuria,
Hypertension : 140/90
and red blood cell (RBC) casts in the Oedema : Facial and Foot edema
urine. This clinical picture is often
accompanied by hypertension, edema,
azotemia
(ie,
decreased
glomerular
filtration rate [GFR]), and renal salt and
water retention. Acute GN can be due to
a primary renal disease or to a systemic
disease.
Epidemiology:
The
incidence
Male, age : 10 years 8 months 13 day
of
acute
glomerulonephritis in patients aged 5-15
years, only 10% occur in patients older
than 40 years. Outbreaks of PSGN are
common in children aged 6-10 years.
Acute nephritis may occur at any age,
including
infancy.
Acute
GN
predominantly affects males (2:1 maleto-female ratio).
Etiology:
Infectious factor :
Serotype-12 Upper Respiratory
Infectious factor
Infection
The most common infectious cause of
acute GN is infection by Streptococcus
species (i.e., group A, beta-hemolytic).
Two
types
have
been
involving different serotypes :
described,
39
Serotype 12 - Poststreptococcal
nephritis due to an upper respiratory
infection.
Serotype 49 - Poststreptococcal
nephritis due to a skin infection
Noninfectious factor
Noninfectious causes of acute GN may
be divided into primary renal diseases
and systemic diseases.
Multisystem systemic diseases:
Vasculitis
Collagen-vascular diseases (e.g,
[SLE])
Hypersensitivity vasculitis
Polyarthritis nodosa
Henoch-Schnlein purpura
Goodpasture syndrome
Primary renal diseases:
Membranoproliferative
glomerulonephritis (MPGN)
Berger Disease (IgA Nephropathy)
Pure mesangial proliferative GN
Idiopathic
rapidly
progressive
glomerulonephritis
Symptoms And Sign:
Patients often have a normal physical
examination and blood pressure. Most
frequently, however, patients present
with
combination
of
edema,
Palpebral and foot oedema
Hypertension : 140/90
Hematuria (+++)
40
hypertension, and oliguria. Some patient
may present the following signs of fluid
overload :
6. Periorbital and/or palpebral edema
7. Edema and hypertension
8. Crackles (i.e., if pulmonary edema)
9. Elevated jugular venous pressure
10. Ascites and pleural effusion
Some patient may present with other
sign, for example :
5. Rash
6. Renal costovertebral fullness or
tenderness
7. Hematuria
8. Abnormal neurologic examination
or altered level of consciousness
Therapy:
Non Pharmacology :
Treatment of glomerulonephritis depend
on whether you have an acute or chronic
form of the disease, the underlying
Bedrest
IVFD D5% 10gtt/i (micro)
Pharmacology :
cause, and the type and severity of your
hours/IV
signs and symptoms. Some cases of
acute
glomerulonephritis,
those
that
follow
Inj. Ondansetron 3mg/12
especially
streptococcus
infection, tend to improve on their own
and often require no specific treatment.
BicNat 1-1-1
Furosemide 2 x 20mg
Valsartan 1 x 20mg
Calnix syrup 3 x Cth I
Adult food low salt low
In general, the goal of treatment is to
protein diet, 1660 kcal with
protect your kidneys from further
56 gr protein
damage.
Keeping
R/ - Dipstick Urine / 6 hours
blood
pressure
under
Urinalysis, Urine Culture
41
control is key to protecting kidneys. To -
C3 Complement, ASTO, CRP
control high blood pressure and slow -
Throat swab
the decline in kidney function, doctor
may
prescribe
one
of
several
medications, including :
-
Diuretics
Angiotensin-converting enzyme
(ACE) inhibitors
Angiotensin II receptor blockers
If there's an underlying cause
for kidney inflammation,
doctor may prescribe other
drugs to treat the underlying
problem, in addition to
treatment to control any
hypertension :
Streptococcus or other bacterial
infection. Your doctor also may
prescribe an appropriate antibiotic.
Lupus or vasculitis. Doctors often
prescribe corticosteroids and
immune-suppressing drugs to
control inflammation.
IgA nephropathy. In some cases,
both fish oil supplements and certain
immune-suppressing drugs can
successfully treat certain people
with IgA nephropathy.
42
Goodpasture's
syndrome. Plasmapheresis is
sometimes used to treat people with
Goodpasture's syndrome.
Prognosis:
Probable good
Most epidemic cases follow a course
ending in complete patient recovery (as
many as 100%). The mortality of acute
GN in the most commonly affected age
group, pediatric patients, has been
reported at 0-7%. Sporadic cases of
acute nephritis often progress to a
chronic form. This progression occurs in
as many as 30% of adult patients and
10% of pediatric patients. GN is the
most common cause of chronic renal
failure (25%).
43
44
CHAPTER 5
SUMMARY
RS, boy aged 10 years 8 months 13 day, came to Haji Adam Malik
Hospital on September 26th, 2016 with chief complaints of red coloured urine. He
was diagnosed with
Acute Kidney Injury Std. Injury e.c.
Acute
Glomerulonephritis + Metabolic Acidosis by history taking, clinical and
laboratory result. He was given a medication both pharmacological and nonpharmacological therapy; such as: Bed Rest, IVFD D5% 4cc / hour (micro), IVFD
NaCl 0,9% 32 gtt/i (micro) for 48 hours, Meylon 29 mEq in D5% 145cc finished
in 4 hours, Inj. Ondansetron 3mg / 12 hours / IV, Inj. Paracetamol 300mg / 8 hours
/ IV, Inj. Ceftriaxone 1gr / 12 hours / IV, Eas Primer 10cc / 12 hours finished in 1
hour, Captopril 2 x 12.5mg, BicNat 2 2 - 2 , KSR 3 x 1 tab Calnix syrup 3 x Cth
I, and Adult Food Low Salt Low Protein Diet, 1600kcal with 56 gr protein. In
October 4th, 2016 the patient was discharged due to his parents willing.
REFERENCES
45
1. Adeva-Andany MM et al. Sodium Bicarbonate Therapy in Patients with
Metabolic Acidosis. The Scientific World Journal; 2014
2. Alatas H. Gagal Ginjal Akut. Kompendium Nefrologi Anak. Jakarta: Ikatan
Dokter Anak Indonesia, 2011 ; 207-214
3. Andreoli SP. Acute kidney Injury in children. Pediatric Nephrology; 2009;
24:253-263
4. Anochie I, Eke F, Okpere A. Childhood acute glomerulonephritis in Port
Harcourt, Rivers State, Nigeria. Niger J Med. 2009 Apr-Jun. 18(2):162-7.
5. Avner ED, Harmon WE, Niaudet P, Yoshikawa N, 2009. Pediatric Nephrology
6th Edition. German: Springer.
6. Baratawidjaja K, Rengganis I. Imunologi Dasar : 8th Edition. Jakarta : 2009.
7. Cohen EP, Sinnakirouchenan R et al, 2014. Nephrotic Syndrome. Accessed
from: http://emedicine.medscape.com/article/244631-overview Last access: 7th
September 2016
8. Ferrario F, Giordano A. Rapidly Progressive Glomerulonephritis. 2010.
9. Fry AC, Farrington K. Management of acute renal failure. Postgrad Med J
2006; 82:106116
10. Guyton A, Hall J. Fisiologi Kedokteran. 2006. 11st Edition.
11. Ibrahim A, Ahmed MM, Bekele D. Clinical profile and outcome of patients
with acute kidney injury requiring dialysis-an experience from a
haemodialysis unit in a developing country. BMC Nephrol. 2016 Jul 22. 17
(1):91.
12. Latief A, Hassan R, Alatas H. Ilmu Kesehatan Anak. Jakarta : 2005
13. Lum MG, editors. Kidney and Urinary Tract, CURRENT Pediatric Diagnosis
& Treatment. 19th Ed. New York : Mc Graw Hill Inc; 2014.
14. Needham E. Management of acute renal failure. American Family Physician
2005;72:1739-46
46
15. Rachmadi D. Gangguan Ginjal Akut. Seminar/ Workshop Nefrologi IDAI
cabang Kaltim, Hotel Aston Balikpapan; 2011.
16. Rauf S, Albar H., Aras J. Konsensus Glomerulonefritis Akut Pasca
Streptokokus. Ikatan Dokter Anak Indonesia. Jakarta : 2012.
17. Schafer E, Schafer A. Immunologic Findings in Glomerulonephritis. 2011.
18. Selewski DT, Symons JM. Acute Kidney Injury. Pediatrics in Review Vol.35
No.1 ; 2014 ; 30-41
19. Sethi S, Fervenza F. Membranoproliferative Glomerulonephritis A New Look
at an Old Entity. 2012.
20. Sudoyo A, Setiyohadi B, Alwi I. Buku Ajar Ilmu Penyakit Dalam. Jakarta :
2009
21. Tjipta G, Ali M, Lubis B. Ragam Pediatrik Praktis. Medan : 2009.
22. Usui J, Tawara-Iida T, Takada K, Ebihara I, Ueda A, Iwabuchi S, et al.
Temporal Changes in Post-Infectious Glomerulonephritis in Japan (19762009). PLoS One. 2016. 11 (6).
23. Vogt, BA, Avner, ED, editors. Renal Failure. 19 th Ed. Philadelphia:
Elsevier/Saunders; 2011.
24. Wong W, Morris MC, Zwi J. Outcome of severe acute post-streptococcal
glomerulonephritis in New Zealand children. Pediatr Nephrol. 2009 May.
24(5):1021-6.
25. Zand L, Nasr S, Sethi S. Membranoproliferative glomerulonephritis
associated with autoimmune diseases. 2014.
You might also like
- Medical TerminologyDocument5 pagesMedical TerminologyjosmdesNo ratings yet
- Management of Diabetic Ketoacidosis in Children and AdolescentsDocument8 pagesManagement of Diabetic Ketoacidosis in Children and AdolescentsnurlatifahNo ratings yet
- National Leaflet About CKD and eGFR For GPs Updated September 2007 PDFDocument2 pagesNational Leaflet About CKD and eGFR For GPs Updated September 2007 PDFRifky Octavio PNo ratings yet
- CPG Management of Dengue Infection in Adults (Revised 2nd Edition)Document68 pagesCPG Management of Dengue Infection in Adults (Revised 2nd Edition)umiraihana1No ratings yet
- DM Renal Plate-3Document5 pagesDM Renal Plate-3api-346187971100% (1)
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiNo ratings yet
- Renal StonesDocument12 pagesRenal StonesDamandeep KaurNo ratings yet
- CRRTDocument12 pagesCRRTPutra RizkiNo ratings yet
- Pre-Op Preparation and Assessment of Pediatric PatientsDocument62 pagesPre-Op Preparation and Assessment of Pediatric PatientsBedahanakugmNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- 1 - Anatomy of The KidneyDocument15 pages1 - Anatomy of The Kidneysara khanNo ratings yet
- HyponatremiaDocument26 pagesHyponatremiaflorenciaii100% (1)
- Hemodialysis ComplicationsDocument10 pagesHemodialysis ComplicationsMuflih NsNo ratings yet
- PD Prescription Present 4-8-52Document74 pagesPD Prescription Present 4-8-52Kong Kong KongNo ratings yet
- AUBF Notes 1Document11 pagesAUBF Notes 1Ice100% (4)
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Critical Care Sepsis Presentation-2Document38 pagesCritical Care Sepsis Presentation-2api-456295176100% (2)
- Vasoactive Agents For Adult Septic Shock: An Update and ReviewDocument10 pagesVasoactive Agents For Adult Septic Shock: An Update and ReviewntnquynhproNo ratings yet
- Biology Notes HSCDocument116 pagesBiology Notes HSCYuki SuzukiNo ratings yet
- Abdominal TuberculosisDocument12 pagesAbdominal TuberculosisBimlesh ThakurNo ratings yet
- Hopkins Medicine Review NephrologyDocument35 pagesHopkins Medicine Review NephrologyMuhammad Bilal50% (2)
- Infective Endocarditis: A Multidisciplinary ApproachFrom EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicNo ratings yet
- Abdominal Aortic Aneurysm and AcuteDocument8 pagesAbdominal Aortic Aneurysm and AcuteKristanto Ayomi Ayomi AriNo ratings yet
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Public Health Nursing: A Textbook for Health Visitors, School Nurses and Occupational Health NursesFrom EverandPublic Health Nursing: A Textbook for Health Visitors, School Nurses and Occupational Health NursesNo ratings yet
- Fluid OverloadDocument19 pagesFluid OverloadfelipebonuttiNo ratings yet
- Acute Renal FailureDocument6 pagesAcute Renal Failurearif kurnia timurNo ratings yet
- Renal Disease in PregnancyDocument28 pagesRenal Disease in PregnancysuperjaxxxonNo ratings yet
- Congenital HerniaDocument5 pagesCongenital HerniaBlazxy EyreNo ratings yet
- A Pictorial Guide For The Second Trimester Ultrasound: EducationDocument16 pagesA Pictorial Guide For The Second Trimester Ultrasound: EducationSultan AlexandruNo ratings yet
- Services Available at Nephrology Department, Serdang HospitalDocument5 pagesServices Available at Nephrology Department, Serdang HospitalASHWEENA A/P SUNDARNo ratings yet
- Taco and Trali: Savita HandayaniDocument12 pagesTaco and Trali: Savita HandayaniAnna Puteri GozaliNo ratings yet
- Overview of The Management of Acute Kidney Injury in Adults - UpToDateDocument13 pagesOverview of The Management of Acute Kidney Injury in Adults - UpToDateDaniely FreitasNo ratings yet
- AKI Vs CKD Lecture Latest 3rd Dec 2018Document51 pagesAKI Vs CKD Lecture Latest 3rd Dec 2018mugilessNo ratings yet
- HydronephrosisDocument6 pagesHydronephrosisJamaluddin Ahmad A.MNo ratings yet
- Intradialytic Hypertension Time To Act 10Document7 pagesIntradialytic Hypertension Time To Act 10Nia FirdiantyNo ratings yet
- Congestive Heart Failure !1 Running Head: Congestive Heart FailureDocument11 pagesCongestive Heart Failure !1 Running Head: Congestive Heart Failureapi-543558169No ratings yet
- Anemia in CKD Patient On HeamodialysisDocument32 pagesAnemia in CKD Patient On HeamodialysisEditor IJTSRDNo ratings yet
- Renal Replacement Therapy in Acute Kidney Injury 2017Document14 pagesRenal Replacement Therapy in Acute Kidney Injury 2017piero reyes100% (1)
- 2017 Hypertension Webinar PDFDocument81 pages2017 Hypertension Webinar PDFMira Mariana UlfahNo ratings yet
- Pharmacology and Physiology in Anesthetic Practice 4e, Robert KDocument2 pagesPharmacology and Physiology in Anesthetic Practice 4e, Robert KSareeya Shre0% (2)
- Management of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesDocument7 pagesManagement of Acute Glomerulonephritis in Children: Children's Services Medical GuidelinesdaypranitaNo ratings yet
- Nephrotic SyndromeDocument14 pagesNephrotic SyndromeAnna Michael AbdullahNo ratings yet
- Nephrology A (Mattheus) : HematuriaDocument10 pagesNephrology A (Mattheus) : HematuriaShekinah MalimbanNo ratings yet
- Guideline, Management of HypernatremiaDocument9 pagesGuideline, Management of HypernatremiaLia Safitri Leloly100% (1)
- Vomiting in Children 2018 PDFDocument19 pagesVomiting in Children 2018 PDFSamuel DiazNo ratings yet
- Peritoneal Dialysis Versus Hemodialysis Risks, Benefits, and Access Issues Clinical SummaryDocument5 pagesPeritoneal Dialysis Versus Hemodialysis Risks, Benefits, and Access Issues Clinical SummaryMarko A. MartínNo ratings yet
- IV Fluid ChartDocument2 pagesIV Fluid Charthady920No ratings yet
- KDIGO AKI Guideline PDFDocument141 pagesKDIGO AKI Guideline PDFAbigail LucasNo ratings yet
- Diagnosis of Gastrointestinal Bleeding in AdultsDocument8 pagesDiagnosis of Gastrointestinal Bleeding in AdultsSaeed Al-YafeiNo ratings yet
- Anemia in CKDDocument149 pagesAnemia in CKDUlises ContrerasNo ratings yet
- Acute Renal FailureDocument12 pagesAcute Renal FailureRifa Aprillia CahyaniNo ratings yet
- What Is IntussusceptionDocument11 pagesWhat Is IntussusceptionNatoya ChristieNo ratings yet
- Kidney TransplantDocument11 pagesKidney TransplantPrincess Xzmae RamirezNo ratings yet
- Horseshoe KidneyDocument26 pagesHorseshoe KidneyarjunjaidevNo ratings yet
- Liver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenDocument79 pagesLiver Cirrhosis: Irish Nicole Dela Cruz Gessel Ann BoguenIrish Nicole DCNo ratings yet
- Pyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaDocument33 pagesPyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaAndaru Tri Setyo WibowoNo ratings yet
- Perioperative Fluid Management in ChildrenDocument31 pagesPerioperative Fluid Management in ChildrenRashmi SahaNo ratings yet
- HydronephrosisDocument15 pagesHydronephrosisAdetz HaedetzNo ratings yet
- Congenital Heart DiseaseDocument124 pagesCongenital Heart DiseasemulkanmustafaNo ratings yet
- Mind Mapping TB in PregnancyDocument1 pageMind Mapping TB in PregnancyAndi Tenri Ola Oddang IINo ratings yet
- Bronchilitis PediatricsDocument10 pagesBronchilitis PediatricsJoseph Arzapalo BenavidesNo ratings yet
- Chronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsDocument7 pagesChronic Kidney Disease : Hypertensive and Diabetic Retinopathy in PatientsAnonymous FgT04krgymNo ratings yet
- PERITONITISDocument27 pagesPERITONITISTiffany Adrias100% (1)
- Acute Pancreatitis - Up To DateDocument31 pagesAcute Pancreatitis - Up To DateNicole AguilarNo ratings yet
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- 3.modern ReviewDocument19 pages3.modern ReviewKrishnaNo ratings yet
- HL Topic 11.3 KidneyDocument6 pagesHL Topic 11.3 KidneyPraveenNo ratings yet
- Microsoft Word - The Urinary SystemDocument19 pagesMicrosoft Word - The Urinary SystemralucaNo ratings yet
- Mineralocorticoid Excess Syndromes: Ellen Marie Freel, Queen Elizabeth University Hospital, Glasgow, United KingdomDocument12 pagesMineralocorticoid Excess Syndromes: Ellen Marie Freel, Queen Elizabeth University Hospital, Glasgow, United KingdomRobby Paguh TariganNo ratings yet
- Case Presentation On CKDDocument13 pagesCase Presentation On CKDCalingalan Hussin Caluang100% (1)
- NephroptosisDocument10 pagesNephroptosisaabbccss1.z71No ratings yet
- Pex 09 02Document4 pagesPex 09 02Haleigh TomaselloNo ratings yet
- Dr. YeshwiniDocument34 pagesDr. YeshwiniSai RakshikaNo ratings yet
- Pharma RenalDocument8 pagesPharma Renalmarlou agananNo ratings yet
- Metabolic Abnormalities in Urinary Diversion Using IntestineDocument16 pagesMetabolic Abnormalities in Urinary Diversion Using IntestineMekbeb ChereNo ratings yet
- Obstructive Nephropathy PDFDocument14 pagesObstructive Nephropathy PDFMuhammad Firdaus J KarimiNo ratings yet
- Assignment 4 PhysioEx 9 2022Document4 pagesAssignment 4 PhysioEx 9 2022Lydia DuncanNo ratings yet
- Case Study #3 Renal 1. LabDocument9 pagesCase Study #3 Renal 1. Labapi-207971474No ratings yet
- General Biology 2 NotesDocument17 pagesGeneral Biology 2 NotesAlyssa Mae BinoNo ratings yet
- Cctarget Multical-Row 1903601 CiblescalibrantDocument6 pagesCctarget Multical-Row 1903601 CiblescalibrantFirman AkoengNo ratings yet
- Acid Base BalanceDocument5 pagesAcid Base Balancemedha chandNo ratings yet
- Chronic GlomerulonephritisDocument18 pagesChronic GlomerulonephritisMarithe Joi Abarico AberosNo ratings yet
- Renap PD CRRTDocument3 pagesRenap PD CRRTHarbyNo ratings yet
- Countercurrent Multiplier and ADHDocument5 pagesCountercurrent Multiplier and ADHAurora TamNo ratings yet
- Regulation of BPDocument17 pagesRegulation of BPLemon CatbaganNo ratings yet