You might also like
- Penn Presby Residency Manual PodiatryDocument400 pagesPenn Presby Residency Manual PodiatryTyler Lawrence Coye100% (1)
- Podiatry Institute ManualDocument301 pagesPodiatry Institute ManualTyler Lawrence Coye100% (2)
- Goljan Step 1 HY 36 Pages Notes PDFDocument36 pagesGoljan Step 1 HY 36 Pages Notes PDFTyler Lawrence CoyeNo ratings yet
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Trauma Manual (Podiatry)Document403 pagesTrauma Manual (Podiatry)QuantumjanitorNo ratings yet
- Anatomy RecallDocument337 pagesAnatomy RecallTyler Lawrence Coye100% (2)
- Operative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Document7 pagesOperative Techniques in Foot and Ankle Surgery - (Axial Screw Technique For Midfoot Arthrodesis in Charcot Foot Deformit... )Tyler Lawrence CoyeNo ratings yet
- Drug Allergy BookDocument332 pagesDrug Allergy Bookmegah_asia13No ratings yet
- Respiratory DrugsDocument6 pagesRespiratory DrugsCurtney PedriaNo ratings yet
- Drugs For Respiratory SystemDocument18 pagesDrugs For Respiratory SystemKaye CorNo ratings yet
- Decongestant - WikipediaDocument7 pagesDecongestant - WikipediaMuhammadafif SholehuddinNo ratings yet
- Respi MedsDocument29 pagesRespi MedsAyesha Calmerin PenuelaNo ratings yet
- By: Cirilo Albert Hicban RN, RMDocument26 pagesBy: Cirilo Albert Hicban RN, RMrongan008No ratings yet
- Asthma 017Document46 pagesAsthma 017Mariam AlavidzeNo ratings yet
- Pain Management in AnimalsDocument46 pagesPain Management in AnimalsSunilNo ratings yet
- Dr. Elly Nurus Sakinah 2010Document23 pagesDr. Elly Nurus Sakinah 2010udunk adhinkNo ratings yet
- Kodex LDocument48 pagesKodex Lamitdwivedi11No ratings yet
- Common ColdDocument4 pagesCommon ColdJohnMyu Beler Jibuy JibuyNo ratings yet
- CoughDocument16 pagesCoughRwapembe StephenNo ratings yet
- Drugs Affecting Respiratory SystemDocument65 pagesDrugs Affecting Respiratory SystemvivianNo ratings yet
- Drugs Affecting Respiratory SystemDocument62 pagesDrugs Affecting Respiratory Systemyunita ekawatiNo ratings yet
- Hyperaldosteronism Is Treated With: Adverse ReactionsDocument7 pagesHyperaldosteronism Is Treated With: Adverse ReactionsGizelle CorpuzNo ratings yet
- Pharmacology Respiratory DrugsDocument2 pagesPharmacology Respiratory DrugsM Youssif Elkady100% (1)
- Pharm5 Common Cold EtiologyDocument5 pagesPharm5 Common Cold EtiologyChristy CorleyNo ratings yet
- Dr. Rishi Pal: Asstt. ProfessorDocument40 pagesDr. Rishi Pal: Asstt. ProfessortamaNo ratings yet
- Drugs Acting On The Respiratory SystemDocument13 pagesDrugs Acting On The Respiratory SystemAlloiBialbaNo ratings yet
- Pulmonary Med Charts Part 2Document2 pagesPulmonary Med Charts Part 2NursingSchoolNotes100% (3)
- Drug List Psych Optho NeuroDocument22 pagesDrug List Psych Optho NeuroAshley BarrileNo ratings yet
- Drugs Affecting The Respiratory System: Antihistamines, Decongestants, Antitussives, and ExpectorantsDocument55 pagesDrugs Affecting The Respiratory System: Antihistamines, Decongestants, Antitussives, and ExpectorantsAli Adan MohamedNo ratings yet
- Drugs Acting On The Pulmonary System 2: Dr. Dita Hasni, M.BiomedDocument24 pagesDrugs Acting On The Pulmonary System 2: Dr. Dita Hasni, M.BiomedYeny ElfiyantiNo ratings yet
- Bronchodilators and Other Respiratory AgentsDocument61 pagesBronchodilators and Other Respiratory Agentsone_nd_onlyuNo ratings yet
- Respiratory System DrugsDocument5 pagesRespiratory System DrugsHamad AlshabiNo ratings yet
- RT Drugs COUGH DIP by ShironDocument6 pagesRT Drugs COUGH DIP by ShironShiron PathiranaNo ratings yet
- Respiratory DrugsDocument22 pagesRespiratory Drugsani bandasoNo ratings yet
- Asthma MedicationDocument6 pagesAsthma Medicationmomina arshidNo ratings yet
- Respiratory Tract PharmacologyDocument68 pagesRespiratory Tract PharmacologyRohaan SharmaNo ratings yet
- Antiasthmatic DrugsDocument36 pagesAntiasthmatic DrugsJannah ZahraaNo ratings yet
- Antiasthmatics and Drugs Used in Cough 2019Document34 pagesAntiasthmatics and Drugs Used in Cough 2019salva sambaaNo ratings yet
- Cough: Cold:: BronchoconstrictionDocument7 pagesCough: Cold:: BronchoconstrictionAbdul MajeedNo ratings yet
- Clinical Pharmacology Reviewer. RespiDocument4 pagesClinical Pharmacology Reviewer. RespiSister RislyNo ratings yet
- Pharmacology 3 Unit 3Document20 pagesPharmacology 3 Unit 3Akshay ShindeNo ratings yet
- Asthma BSPDocument34 pagesAsthma BSPÁnh PhạmNo ratings yet
- Drugs Acting On Respiratory SystemDocument3 pagesDrugs Acting On Respiratory SystemAlyssa Audrey CaoagasNo ratings yet
- Respratory Drugs I-IIDocument10 pagesRespratory Drugs I-IITyler Lawrence CoyeNo ratings yet
- Acute Asthma Exacerbations: DR Abdelmoniem Saeed Mohammed Er SpecialistDocument36 pagesAcute Asthma Exacerbations: DR Abdelmoniem Saeed Mohammed Er SpecialistYousef Al-AmeenNo ratings yet
- Respiratory DrugsDocument56 pagesRespiratory DrugsIra G. Delos Santos100% (1)
- Respi DrugsDocument36 pagesRespi DrugsLady Mae RamosNo ratings yet
- Defn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andDocument5 pagesDefn: Periodic Spasm of Bronchial Smooth Muscles, Increased Secretion, andSambit BeheraNo ratings yet
- COPDwith Steroidsand BronchodilatorsDocument3 pagesCOPDwith Steroidsand BronchodilatorsTom MallinsonNo ratings yet
- Drugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedDocument32 pagesDrugs Affecting The Respiratory Systems: Kuntarti, SKP, MbiomedRichard BungaNo ratings yet
- Bronchodilator & Other Drugs Used in AsthmaDocument15 pagesBronchodilator & Other Drugs Used in AsthmaGenta JagadNo ratings yet
- Drugs Acting On Respiratory System 6640Document137 pagesDrugs Acting On Respiratory System 6640Umar Bakshi100% (1)
- Group 3 Respiratory SystemDocument69 pagesGroup 3 Respiratory Systemgoodemonz15No ratings yet
- Drugs For Asthma, COPD, GIT, DyslipidemiaDocument163 pagesDrugs For Asthma, COPD, GIT, DyslipidemiaPatricia ManaliliNo ratings yet
- Asma by HendraDocument37 pagesAsma by HendraAl SyarfinaNo ratings yet
- Printed Material ModuleeeeDocument56 pagesPrinted Material ModuleeeeShang MacarayonNo ratings yet
- Asthma + COPDDocument60 pagesAsthma + COPDNur HasanahNo ratings yet
- Urti Lrti Drugs 2023Document8 pagesUrti Lrti Drugs 2023dlabdon0310No ratings yet
- Pharmacology Chapter 26 - Respiratory DrugsDocument19 pagesPharmacology Chapter 26 - Respiratory DrugsEnrique Guillen InfanteNo ratings yet
- Lecture 4, 5 - Drugs Used in Bronchial Asthma & COPDDocument57 pagesLecture 4, 5 - Drugs Used in Bronchial Asthma & COPDBalakrishnan Thangaraj100% (1)
- Respiratory Drugs 2Document4 pagesRespiratory Drugs 2Ella RivaNo ratings yet
- Drugs Acting On The Pulmonary System 1: Dr. Dita Hasni, M.BiomedDocument50 pagesDrugs Acting On The Pulmonary System 1: Dr. Dita Hasni, M.BiomedYeny ElfiyantiNo ratings yet
- 3 ParasympatholyticsDocument35 pages3 ParasympatholyticsSudhakar LakavathNo ratings yet
- Analgesia and AnalgesicsDocument113 pagesAnalgesia and Analgesicsdr_shilpakokate9368No ratings yet
- BeclomethasoneDocument1 pageBeclomethasoneMuhammad ArsalanNo ratings yet
- Athma, COPD and Cough AgentsDocument71 pagesAthma, COPD and Cough AgentsBriana NdayisabaNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- READMEDocument1 pageREADMETyler Lawrence CoyeNo ratings yet
- Meta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingDocument21 pagesMeta-Analysis of Diagnostic Accuracy With Mada: Philipp Doebler Heinz HollingTyler Lawrence CoyeNo ratings yet
- Dfa 6 29629Document12 pagesDfa 6 29629Tyler Lawrence CoyeNo ratings yet
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Document3 pagesLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyeNo ratings yet
- Jfas Original ResearchDocument12 pagesJfas Original ResearchTyler Lawrence CoyeNo ratings yet
- Trauma Workshop 1Document10 pagesTrauma Workshop 1Tyler Lawrence CoyeNo ratings yet
- Treatment of Lisfranc Fracture-Dislocations With PDocument8 pagesTreatment of Lisfranc Fracture-Dislocations With PTyler Lawrence CoyeNo ratings yet
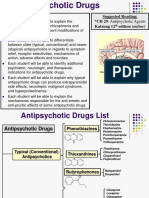
- AntipsychoticsDocument29 pagesAntipsychoticsTyler Lawrence Coye100% (5)
- Ankle Instability 2017-2018Document44 pagesAnkle Instability 2017-2018Tyler Lawrence CoyeNo ratings yet
- Crozer Manual - Second Edition PDFDocument219 pagesCrozer Manual - Second Edition PDFTyler Lawrence CoyeNo ratings yet
- Lecture-12-2 22 17Document7 pagesLecture-12-2 22 17Tyler Lawrence CoyeNo ratings yet
- 16 Principles of Ankle and Foot CTDocument48 pages16 Principles of Ankle and Foot CTTyler Lawrence CoyeNo ratings yet
- Lecture 3 Capsule Tendon Balance ProceduresDocument19 pagesLecture 3 Capsule Tendon Balance ProceduresTyler Lawrence CoyeNo ratings yet
- 09 Vascular TraumaDocument36 pages09 Vascular TraumaTyler Lawrence CoyeNo ratings yet
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocument16 pagesThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Anti EpilepticsDocument46 pagesAnti EpilepticsTyler Lawrence CoyeNo ratings yet
- AnticoagulantsDocument47 pagesAnticoagulantsTyler Lawrence Coye100% (1)
- Respratory Drugs I-IIDocument10 pagesRespratory Drugs I-IITyler Lawrence CoyeNo ratings yet
- Venous DiseaseDocument19 pagesVenous DiseaseTyler Lawrence CoyeNo ratings yet
- Wound and Skin Ulcer Management Care Guide PDFDocument21 pagesWound and Skin Ulcer Management Care Guide PDFAdriel Chandra AngNo ratings yet
- The Ohio Book - LEA DiagramsDocument168 pagesThe Ohio Book - LEA DiagramsTyler Lawrence Coye100% (2)
- Chapter 8 - Head and Neck 2015Document72 pagesChapter 8 - Head and Neck 2015Tyler Lawrence CoyeNo ratings yet
- Mit PDFDocument106 pagesMit PDFTyler Lawrence CoyeNo ratings yet
- Respiratory Agents.2015Document75 pagesRespiratory Agents.2015sarwatNo ratings yet
- Pathophysiology of AsthmaDocument2 pagesPathophysiology of AsthmaAhyz100% (3)
- Farmakologi Antihistamin-RDY 2019Document50 pagesFarmakologi Antihistamin-RDY 2019fandi mnNo ratings yet
- Zakiudin Munasir - Food Allergy and ManifestationDocument32 pagesZakiudin Munasir - Food Allergy and ManifestationernitaNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic Rhinitispaningbatan.kristine.bNo ratings yet
- Sci 3 NC 328 F3 Bru 4 Ry 2014Document133 pagesSci 3 NC 328 F3 Bru 4 Ry 2014george_scalaNo ratings yet
- This Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eDocument4 pagesThis Study Resource Was: Dlugasch - Ch02-Applied Pathophysiology For The Advanced Practice Nurse, 1eHugs0% (1)
- International Journal of Pharmtech ResearchDocument5 pagesInternational Journal of Pharmtech Researchrosnita sidabalokNo ratings yet
- 1st LE MedicineDocument11 pages1st LE MedicineDia DimayugaNo ratings yet
- Hypersensitivity Reactions (Immunologic Tissue Injury)Document17 pagesHypersensitivity Reactions (Immunologic Tissue Injury)Revathi NerusuNo ratings yet
- RISPDocument149 pagesRISPDessu AshagrieNo ratings yet
- Asthma, Obesity, and Microbiota - A Complex Immunological InteractionDocument33 pagesAsthma, Obesity, and Microbiota - A Complex Immunological InteractionMarcelo CosendeyNo ratings yet
- Old Immunology Exam(s)Document16 pagesOld Immunology Exam(s)Ham Mad0% (1)
- Paper 8690Document8 pagesPaper 8690IJARSCT JournalNo ratings yet
- BT102-Microbiology Current Paper Solved Question Final Term February 2020Document11 pagesBT102-Microbiology Current Paper Solved Question Final Term February 2020Awais Bhutta100% (1)
- Jurnal Rhinitis Alergi PDFDocument8 pagesJurnal Rhinitis Alergi PDFAyuindiraNo ratings yet
- Book-Based: Pathophysiology of Allergic RhinitisDocument2 pagesBook-Based: Pathophysiology of Allergic RhinitisJeraldine Corpuz PascualNo ratings yet
- (Advances in Food and Nutrition Research Volume 73) Kim, Se-Kwon-Marine Carbohydrates - Fundamentals and Applications, Part B-ADocument291 pages(Advances in Food and Nutrition Research Volume 73) Kim, Se-Kwon-Marine Carbohydrates - Fundamentals and Applications, Part B-ASugiyanto GunadiNo ratings yet
- 2020 Anaphylaxis JACI 2020Document42 pages2020 Anaphylaxis JACI 2020Peter Albeiro Falla CortesNo ratings yet
- Atopy - StatPearls - NCBI Bookshelf PDFDocument10 pagesAtopy - StatPearls - NCBI Bookshelf PDFAikawa MitaNo ratings yet
- Prof Iwin - Asit Course Final Method and Its Eval Exp 30' JKT Feb 08Document79 pagesProf Iwin - Asit Course Final Method and Its Eval Exp 30' JKT Feb 08nick_mdNo ratings yet
- Allergic RhinitisDocument19 pagesAllergic RhinitisNicole Villaflor FabicoNo ratings yet
- Jurnal AlergiDocument9 pagesJurnal AlergiNana MuktiNo ratings yet
- Westie Heal The BookDocument177 pagesWestie Heal The BookNemo Westie Ogi IINo ratings yet
- Doxicyclin and AcnesDocument23 pagesDoxicyclin and AcnesRafiqy Sa'adiy FaizunNo ratings yet
- An Introduction To Antibodies and Their ApplicationsDocument100 pagesAn Introduction To Antibodies and Their ApplicationsAlessandroNo ratings yet
- Differential Release of Mast Cell Mediators and The Pathogenesis of InflammationDocument14 pagesDifferential Release of Mast Cell Mediators and The Pathogenesis of InflammationklaumrdNo ratings yet
- Anaphylactic ShockDocument36 pagesAnaphylactic ShockCarmelli Mariae Calugay100% (1)
- 2022 Article 688Document12 pages2022 Article 688fatima amaliaNo ratings yet

































































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)