You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Benefits and Risks of Antiretroviral TherapyDocument12 pagesBenefits and Risks of Antiretroviral TherapyAtgy Dhita AnggraeniNo ratings yet
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- Activation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment DoveDocument16 pagesActivation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment Dovemr dexterNo ratings yet
- Ulkus Kornea Eng VerDocument15 pagesUlkus Kornea Eng VerDexter BluesNo ratings yet
- QuestionsDocument1 pageQuestionsDexter BluesNo ratings yet
- Medi 96 E5795 PDFDocument5 pagesMedi 96 E5795 PDFDexter BluesNo ratings yet
- Pamj 24 182 PDFDocument5 pagesPamj 24 182 PDFDexter BluesNo ratings yet
- Nejmoa1514762 PDFDocument12 pagesNejmoa1514762 PDFDexter BluesNo ratings yet
- SDJ 2016 09 01 PDFDocument7 pagesSDJ 2016 09 01 PDFDexter BluesNo ratings yet
- Jurnal Anak Ririn PDFDocument10 pagesJurnal Anak Ririn PDFDexter BluesNo ratings yet
- Nejmoa1606356 PDFDocument10 pagesNejmoa1606356 PDFDexter BluesNo ratings yet
- Fix ObgynDocument17 pagesFix ObgynDexter BluesNo ratings yet
- PRM2016 1658172 PDFDocument7 pagesPRM2016 1658172 PDFDexter BluesNo ratings yet
- Jurnal Anak RirinDocument10 pagesJurnal Anak RirinDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- Mood Dynamics in Bipolar Disorder: Research Open AccessDocument9 pagesMood Dynamics in Bipolar Disorder: Research Open AccesswulanfarichahNo ratings yet
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- 1830 PDF PDFDocument5 pages1830 PDF PDFDexter BluesNo ratings yet
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
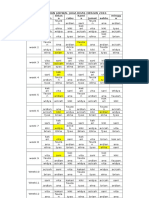
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDocument1 pageRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument3 pagesThe Seven Cardinal MovementsMaria Mandid0% (1)
- Pruritus: An Updated Look at An Old ProblemDocument7 pagesPruritus: An Updated Look at An Old ProblemThariq Mubaraq DrcNo ratings yet
- Unchallengeable Miracles of QuranDocument430 pagesUnchallengeable Miracles of QuranyoursincerefriendNo ratings yet
- 10 4103@0378-6323 116725 PDFDocument14 pages10 4103@0378-6323 116725 PDFDexter BluesNo ratings yet
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNo ratings yet
- Geriatric Itch PDFDocument16 pagesGeriatric Itch PDFDexter BluesNo ratings yet
- Jurnal Elderly 2 PDFDocument3 pagesJurnal Elderly 2 PDFDexter BluesNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- What Is Mindfulness?Document2 pagesWhat Is Mindfulness?Vaseem SyedNo ratings yet
- A Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESDocument57 pagesA Case Presentation On:: Bipolar 1 Disorder, MRE With Psychotic FEARURESLane Mae Magpatoc NoerrotNo ratings yet
- Case Report OEDDocument7 pagesCase Report OEDarief ardaNo ratings yet
- Suspension Therapy by Rahul Vapms CopDocument20 pagesSuspension Therapy by Rahul Vapms Copvenkata ramakrishnaiahNo ratings yet
- Five Theories of Human ExistenceDocument6 pagesFive Theories of Human ExistenceQuenine BridgeNo ratings yet
- Larry Nassar Ingham County AffidavitDocument5 pagesLarry Nassar Ingham County AffidavitDeadspinNo ratings yet
- HeartsInHarmony PDFDocument103 pagesHeartsInHarmony PDFVanessa100% (9)
- Practical Research 2: "Correlation of Anxiety To Students' Achievement"Document4 pagesPractical Research 2: "Correlation of Anxiety To Students' Achievement"Marie LargoNo ratings yet
- Case AnaDocument12 pagesCase AnaBiel DelcanoNo ratings yet
- CHF PathophysiologyDocument4 pagesCHF PathophysiologyVirtudazo JessaNo ratings yet
- Ws Viii Dyspepsia - Dr. Ignatia Sinta Murti, SP - Pd-KgehDocument79 pagesWs Viii Dyspepsia - Dr. Ignatia Sinta Murti, SP - Pd-KgehSriHandaryatiNo ratings yet
- NFDN 2003-2Document3 pagesNFDN 2003-2api-306019377100% (1)
- Essential Oils A Handbook For Aromatherapy PracticeDocument321 pagesEssential Oils A Handbook For Aromatherapy PracticeDenisa Florea100% (54)
- Med SurgDocument38 pagesMed SurgEm Israel Jr.No ratings yet
- Clinical FormulationDocument24 pagesClinical Formulationaimee2oo8100% (2)
- Cognitive & Behavioral Therapy: (Clinical Psychology)Document3 pagesCognitive & Behavioral Therapy: (Clinical Psychology)Nowella Kryzel PelayoNo ratings yet
- Soap NoteDocument2 pagesSoap Noteapi-285542134No ratings yet
- Transactional Analysis: Understanding Behavior Through Parent, Adult, Child TheoryDocument1 pageTransactional Analysis: Understanding Behavior Through Parent, Adult, Child TheoryForam ShahNo ratings yet
- Perioperative CareDocument48 pagesPerioperative CareBryan FederizoNo ratings yet
- Jurnal Enzim AmilaseDocument6 pagesJurnal Enzim AmilaseTriRatnaFauziahNo ratings yet
- Hot Stone Massage BenefitsjhxnjDocument2 pagesHot Stone Massage Benefitsjhxnjsecondstove31No ratings yet
- Artificial AirwaysDocument17 pagesArtificial AirwaysSri DarmayantiNo ratings yet
- QigongDocument12 pagesQigongCarlos EdreiraNo ratings yet
- Heritage Village ProjectDocument24 pagesHeritage Village ProjectHaindava Keralam50% (2)
- Mitchell, Carol - ResumeDocument2 pagesMitchell, Carol - Resumeapi-238460511No ratings yet
- Dosis Oseltamivir CDCDocument3 pagesDosis Oseltamivir CDCivonne marinNo ratings yet
- The Core Conflictual Relationship Theme Applied To Literary WorksDocument11 pagesThe Core Conflictual Relationship Theme Applied To Literary WorksPamela Francisca Bobadilla BurgosNo ratings yet
- Pharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsDocument7 pagesPharmacokinetics and pharmacodynamics of anaesthetic drugs in paediatricsR KNo ratings yet
- Ayurveda ExtractionDocument9 pagesAyurveda ExtractionDr-Beneesh VK0% (1)
- ALSANGEDY BULLETS For PACES Ankylosing Spondylitis 2nd EditionDocument2 pagesALSANGEDY BULLETS For PACES Ankylosing Spondylitis 2nd EditionGhulamMemonNo ratings yet