You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- AWS March, 2018Document16 pagesAWS March, 2018Fazal MalikNo ratings yet
- Fazal CVDocument3 pagesFazal CVFazal MalikNo ratings yet
- Details of Major Hospitals: S.No Name of HospitalDocument2 pagesDetails of Major Hospitals: S.No Name of HospitalFazal MalikNo ratings yet
- Master Contact & Prescriber List: AM600 Plt-50 Plt100 ProtnDocument106 pagesMaster Contact & Prescriber List: AM600 Plt-50 Plt100 ProtnFazal MalikNo ratings yet
- Monthly Report For Doppler Program RevDocument2 pagesMonthly Report For Doppler Program RevFazal MalikNo ratings yet
- Marketing EthicsDocument16 pagesMarketing EthicsFazal MalikNo ratings yet
- Pharmaceutical MarketingDocument6 pagesPharmaceutical MarketingFazal MalikNo ratings yet
- Is Your Sales Organization Good or Great?: Harvard Business ReviewDocument2 pagesIs Your Sales Organization Good or Great?: Harvard Business ReviewFazal MalikNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Antibiotic Resistance Gene Testing of Recycled Water Samples in Flagstaff, AZDocument7 pagesAntibiotic Resistance Gene Testing of Recycled Water Samples in Flagstaff, AZkrtica8061No ratings yet
- Central Line Infection PathwayDocument36 pagesCentral Line Infection PathwayAnonymous 9dVZCnTXSNo ratings yet
- دوائيات ن- lec22-ReducedDocument24 pagesدوائيات ن- lec22-Reducedma22mdmmNo ratings yet
- Stock L5-1Document1 pageStock L5-1wisnubernofarmNo ratings yet
- Antibiotic EssentialsDocument6 pagesAntibiotic EssentialsAna MariaNo ratings yet
- Antibacterial Agents NotesDocument6 pagesAntibacterial Agents NotesschxzerrydawnNo ratings yet
- Drugs ListDocument195 pagesDrugs ListAmit Kumar100% (3)
- Burkholderia CepaciaDocument3 pagesBurkholderia Cepaciavecerzan_lilianaNo ratings yet
- Drug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityDocument1 pageDrug Dosage Mechanism of Action Indications & Contraindications Side Effects & Adverse Effects Nursing ResponsibilityAthena SaturdayNo ratings yet
- First Draft Phage TherapyDocument16 pagesFirst Draft Phage Therapyapi-324155293No ratings yet
- Cefazolin and Dextrose USPDocument3 pagesCefazolin and Dextrose USPYaleswari Hayu PertiwiNo ratings yet
- Phytopharmalogical Significance of Terminalia Catappa An Updated ReviewDocument8 pagesPhytopharmalogical Significance of Terminalia Catappa An Updated ReviewYonita Yuliani100% (1)
- Extended Infusion Meropenem Protocol PDFDocument5 pagesExtended Infusion Meropenem Protocol PDFAbu Hammoud AlyazeediNo ratings yet
- Mic MBCDocument5 pagesMic MBCOneil CerdenaNo ratings yet
- DR - Dash Profile Nutra Now 14 PDFDocument19 pagesDR - Dash Profile Nutra Now 14 PDFChintalaRaoNo ratings yet
- Media Preparation ProtocolDocument5 pagesMedia Preparation ProtocolmohdkhairNo ratings yet
- Bauer 2019Document6 pagesBauer 2019RaffaharianggaraNo ratings yet
- 21 CFR 558.15 "Studies": A Brief History: Jeffrey M. Gilbert, PH.DDocument24 pages21 CFR 558.15 "Studies": A Brief History: Jeffrey M. Gilbert, PH.Drosebelle1906No ratings yet
- Urological Infections 2010.PDF EditDocument112 pagesUrological Infections 2010.PDF EditMuhammad Bilal Bin AmirNo ratings yet
- DGFT Public Notice No.64/2015-2020 Dated 17th March, 2015Document3 pagesDGFT Public Notice No.64/2015-2020 Dated 17th March, 2015stephin k jNo ratings yet
- USPI - Bicillin C-R - Penicillin G Benzathine, Penicillin GDocument11 pagesUSPI - Bicillin C-R - Penicillin G Benzathine, Penicillin GRoberto Alfredo SáenzNo ratings yet
- Salinan Dari Jadwal KF Kedung CowekDocument47 pagesSalinan Dari Jadwal KF Kedung Cowekdwikamaliyatissholehah94No ratings yet
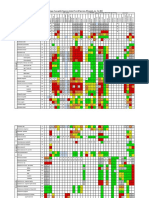
- Organism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020Document2 pagesOrganism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020BaronKornNo ratings yet
- HJNHNNDocument9 pagesHJNHNNProbioticsAnywhereNo ratings yet
- Aus Pi TargocidDocument5 pagesAus Pi TargocidAsto Ata InteristiNo ratings yet
- Antibiotic TableDocument5 pagesAntibiotic TableLiana Et Murat KalabalikNo ratings yet
- Jurnal Reading OsteomyelitisDocument11 pagesJurnal Reading Osteomyelitisfidela_ffNo ratings yet
- Achyranthes Aspera PDFDocument7 pagesAchyranthes Aspera PDFzenith492No ratings yet
- Pattern of Researches Done On Antimicrobial Resistance in EthiopiaDocument16 pagesPattern of Researches Done On Antimicrobial Resistance in EthiopiaandualemNo ratings yet
- Panchavakala Kwath Antimicrobial Activity of Ayurvedic Hand SanitizersDocument5 pagesPanchavakala Kwath Antimicrobial Activity of Ayurvedic Hand SanitizersUmeshNo ratings yet