You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Asthma PathophysiologyDocument1 pageAsthma PathophysiologyElisa Kerr100% (2)
- Bachelor of Science Biomedical ScienceDocument1 pageBachelor of Science Biomedical SciencePasipanodya Muzenda100% (1)
- Mantoux TestDocument3 pagesMantoux Testfarrukhhussain2006No ratings yet
- Community Herbal MedicineDocument4 pagesCommunity Herbal MedicineMary Joyce Ariem100% (1)
- Workplace Site Audit Checklist PharmacyDocument3 pagesWorkplace Site Audit Checklist PharmacyWaqar LatifNo ratings yet
- Blood Pressure ChartDocument5 pagesBlood Pressure Chartmahajan1963100% (1)
- Related LitDocument8 pagesRelated LitElisa KerrNo ratings yet
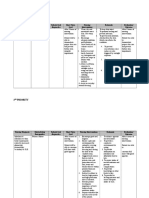
- Acs NCPDocument3 pagesAcs NCPElisa KerrNo ratings yet
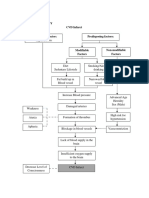
- CVD PathoohysiologyDocument1 pageCVD PathoohysiologyElisa KerrNo ratings yet
- Systemic Lupuc ErthymosusDocument3 pagesSystemic Lupuc ErthymosusElisa KerrNo ratings yet
- Nursing care plan for skin lesions, nutrition, and activity toleranceDocument3 pagesNursing care plan for skin lesions, nutrition, and activity toleranceElisa Kerr100% (1)
- Bronchial Asthma PathophysiologyDocument1 pageBronchial Asthma PathophysiologyElisa Kerr100% (2)
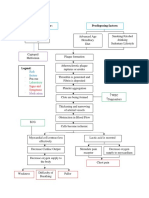
- Risk Factors and Processes Leading to Myocardial InfarctionDocument1 pageRisk Factors and Processes Leading to Myocardial InfarctionElisa KerrNo ratings yet
- Acute Gout Case StudyDocument2 pagesAcute Gout Case StudyElisa KerrNo ratings yet
- Safe and Effective CareDocument4 pagesSafe and Effective CareElisa KerrNo ratings yet
- Pathophysiology CVD InfarctDocument1 pagePathophysiology CVD InfarctElisa KerrNo ratings yet
- SchizophreniaDocument7 pagesSchizophreniaElisa KerrNo ratings yet
- Notification Letter EnglishDocument1 pageNotification Letter EnglishJovele OctobreNo ratings yet
- Penerapan E-Resep Meningkatkan Mutu Farmasi RS di JakartaDocument5 pagesPenerapan E-Resep Meningkatkan Mutu Farmasi RS di JakartaIim RimbaNo ratings yet
- Impetigo in NeonatusDocument5 pagesImpetigo in Neonatusasep budiyantoNo ratings yet
- EEReview PDFDocument7 pagesEEReview PDFragavendharNo ratings yet
- Adolescent Health and Youth ProgramDocument77 pagesAdolescent Health and Youth ProgramRijane Tabonoc OmlangNo ratings yet
- MCQ 23Document10 pagesMCQ 23Old driverNo ratings yet
- Tarsal Tunnel SyndromeDocument2 pagesTarsal Tunnel SyndromeMuhammad Amri KautsarNo ratings yet
- General AnaestheticDocument10 pagesGeneral AnaestheticFeyaNo ratings yet
- Under Guidance of Mr. Mali K.K. (Assistant Professor) : 1 Yspm, YtcDocument41 pagesUnder Guidance of Mr. Mali K.K. (Assistant Professor) : 1 Yspm, YtcSabiruddin Mirza DipuNo ratings yet
- De Vries Et Al. (1998) and Bolman & de Vries (1998)Document2 pagesDe Vries Et Al. (1998) and Bolman & de Vries (1998)Anonymous 8rsxG4No ratings yet
- 3 Most Common Biochemical ImbalancesDocument4 pages3 Most Common Biochemical Imbalancescarlos100% (1)
- Corresponding Author: Dr. K. Ramu, Hemalatha .S 1.principalDocument5 pagesCorresponding Author: Dr. K. Ramu, Hemalatha .S 1.principalBalaMuruganNo ratings yet
- The Open Dentistry Journal: The Effect of Chin-Cup Therapy in Class III Malocclusion: A Systematic ReviewDocument16 pagesThe Open Dentistry Journal: The Effect of Chin-Cup Therapy in Class III Malocclusion: A Systematic ReviewmilanmashrukNo ratings yet
- Why Bladder Training Prior To Foley Catheter Removal Is Not BestDocument10 pagesWhy Bladder Training Prior To Foley Catheter Removal Is Not BestManoj KumarNo ratings yet
- Mixed Connective Tissue DZ (SLE + Scleroderma)Document7 pagesMixed Connective Tissue DZ (SLE + Scleroderma)AshbirZammeriNo ratings yet
- Expanded Mobile Crisis Outreach Team (EMCOT)Document3 pagesExpanded Mobile Crisis Outreach Team (EMCOT)Kyle A McCallNo ratings yet
- Asclepius Consulting IntroductionDocument3 pagesAsclepius Consulting Introductionapi-3710510No ratings yet
- Medical and Dental Clearance.1 2017Document2 pagesMedical and Dental Clearance.1 2017cristina tamonteNo ratings yet
- COVID-19 Environmental Health and Safety PlanDocument23 pagesCOVID-19 Environmental Health and Safety PlanolaogunNo ratings yet
- Cancer Ms LecDocument16 pagesCancer Ms LecJulia Rae Delos Santos100% (1)
- Presented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinDocument36 pagesPresented by Animesh Amal: Brand Plan On Salbutamol + Ambroxol + GuaifenesinAnonymous 75aETJ8ONo ratings yet
- Urgent: Invented by William H. Gates (Aka Bill Gates) and Others, Listing Energy HarvestingDocument3 pagesUrgent: Invented by William H. Gates (Aka Bill Gates) and Others, Listing Energy HarvestingShayna A PitreNo ratings yet
- Tube+Aftercare+Tear Off+Sheets+PDFDocument8 pagesTube+Aftercare+Tear Off+Sheets+PDFNikola StojsicNo ratings yet
- AO CMFS During COVID-19Document6 pagesAO CMFS During COVID-19โสภาพรรณวดี รวีวารNo ratings yet
- Shalu Bathla - Chronic PeriodontitisDocument6 pagesShalu Bathla - Chronic PeriodontitisFerdinan PasaribuNo ratings yet