You might also like
- Sd. de Caídas - 2017 - Problemas de Balance y RiesgosDocument11 pagesSd. de Caídas - 2017 - Problemas de Balance y RiesgosManuel MontellanosNo ratings yet
- SD de Caídas - 2018 - Hipnóticos No Benzodiacepínicos Asoc A Caídas en AsiloDocument9 pagesSD de Caídas - 2018 - Hipnóticos No Benzodiacepínicos Asoc A Caídas en AsiloManuel MontellanosNo ratings yet
- Vitamina D - Mortalidad Prematura - EdadDocument18 pagesVitamina D - Mortalidad Prematura - EdadManuel MontellanosNo ratings yet
- Anafilaxia 2010Document46 pagesAnafilaxia 2010lilicasrNo ratings yet
- Guitar 1994-01Document55 pagesGuitar 1994-01Magdalena Głowa100% (6)
- Amiloidosis - DXDocument11 pagesAmiloidosis - DXManuel MontellanosNo ratings yet
- CVC - 2017 - Que Tan Seguro Es X EcografíaDocument6 pagesCVC - 2017 - Que Tan Seguro Es X EcografíaManuel MontellanosNo ratings yet
- Adherencia A Práctica ClínicaDocument8 pagesAdherencia A Práctica ClínicaManuel MontellanosNo ratings yet
- Constipacion - 2017 - Regimen Intestinal - EnseñanzaDocument2 pagesConstipacion - 2017 - Regimen Intestinal - EnseñanzaManuel MontellanosNo ratings yet
- EKG - 2017 - Taquiarritmia y TelimetríaDocument3 pagesEKG - 2017 - Taquiarritmia y TelimetríaManuel MontellanosNo ratings yet
- Desequilibrio Acidobase7 PDFDocument8 pagesDesequilibrio Acidobase7 PDFManuel MontellanosNo ratings yet
- Hta Sal Sensible - Rol RiñonDocument6 pagesHta Sal Sensible - Rol RiñonManuel MontellanosNo ratings yet
- CA de Ovario - HistoriaDocument1 pageCA de Ovario - HistoriaManuel MontellanosNo ratings yet
- TVP - Tto Ambulatorio - ComorbilidadDocument6 pagesTVP - Tto Ambulatorio - ComorbilidadManuel MontellanosNo ratings yet
- CA Hepático - Quimioterapia NeoadyuvanteDocument16 pagesCA Hepático - Quimioterapia NeoadyuvanteManuel MontellanosNo ratings yet
- ICU sedation guide for commonly used analgesics and sedativesDocument19 pagesICU sedation guide for commonly used analgesics and sedativesManuel MontellanosNo ratings yet
- Pneumotorax Recurrente - DermatomiositisDocument3 pagesPneumotorax Recurrente - DermatomiositisManuel MontellanosNo ratings yet
- ACV Isquémico - 2015 - Hipocampo Bilateral Por CocaínaDocument3 pagesACV Isquémico - 2015 - Hipocampo Bilateral Por CocaínaManuel MontellanosNo ratings yet
- Calcificación Vascular - 2016 - Inflamación Acelerada - TtoDocument10 pagesCalcificación Vascular - 2016 - Inflamación Acelerada - TtoManuel MontellanosNo ratings yet
- Atropina Uso en OrganofosforadosDocument6 pagesAtropina Uso en OrganofosforadosManuel MontellanosNo ratings yet
- Carcinoma Associated Paraneoplastic PeriDocument8 pagesCarcinoma Associated Paraneoplastic PeriManuel MontellanosNo ratings yet
- Café - 2016 - Primera CienciaDocument1 pageCafé - 2016 - Primera CienciaManuel MontellanosNo ratings yet
- Tos Cronica Articulo NejmDocument8 pagesTos Cronica Articulo NejmEdwin CvNo ratings yet
- Meningioma - 1998 - AIT o Deficit Neurologico TransitorioDocument5 pagesMeningioma - 1998 - AIT o Deficit Neurologico TransitorioManuel MontellanosNo ratings yet
- Acalasia - TratamientoDocument6 pagesAcalasia - TratamientoManuel MontellanosNo ratings yet
- DM - FC RX CV - CTRL MetabDocument18 pagesDM - FC RX CV - CTRL MetabManuel MontellanosNo ratings yet
- Meningioma - 1994 - AIT - Reporte de 4 CasosDocument3 pagesMeningioma - 1994 - AIT - Reporte de 4 CasosManuel MontellanosNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Professional Development PowerpointDocument11 pagesProfessional Development Powerpointapi-507364479No ratings yet
- Vaccination Program in Farm AnimalDocument87 pagesVaccination Program in Farm AnimalThành Đỗ MinhNo ratings yet
- dwn150082F ns210 1602080177Document9 pagesdwn150082F ns210 1602080177Cindy ParamitaaNo ratings yet
- Physiotherapy Functional Assessment GridDocument2 pagesPhysiotherapy Functional Assessment GridILR 2019No ratings yet
- Guidelines For Preventing HealthcareDocument78 pagesGuidelines For Preventing HealthcareppeterarmstrongNo ratings yet
- Deficient Fluid Volume (AGEDocument2 pagesDeficient Fluid Volume (AGENursesLabs.com83% (6)
- Chapter 9 KeyDocument17 pagesChapter 9 KeySrinu WestNo ratings yet
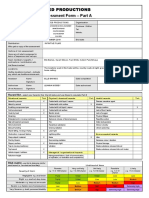
- Twisted Risk Assesment 2Document2 pagesTwisted Risk Assesment 2api-306671250100% (1)
- Module 1: Disability, Inequality, and InclusionDocument25 pagesModule 1: Disability, Inequality, and InclusionAuberon Jeleel OdoomNo ratings yet
- Shubitz Family Clinic Info Sheet - 2016Document2 pagesShubitz Family Clinic Info Sheet - 2016api-233269901No ratings yet
- An Overview of Asthma Management - UpToDateDocument31 pagesAn Overview of Asthma Management - UpToDateSantiago Mondragon RiosNo ratings yet
- Answer Key CicDocument3 pagesAnswer Key Cictiburshoc16No ratings yet
- Product B - Edhawa Herbal MedicineDocument3 pagesProduct B - Edhawa Herbal MedicineJae Tuffie KatneesNo ratings yet
- Research Methods Final PaperDocument18 pagesResearch Methods Final Paperapi-449754716No ratings yet
- Lukeka Shabani Papy-CVDocument3 pagesLukeka Shabani Papy-CVAnonymous o32OUFNo ratings yet
- Well Fact Sheet: Suitability of Water For Livestock Fact SheetDocument2 pagesWell Fact Sheet: Suitability of Water For Livestock Fact SheetHill County Conservation DistrictNo ratings yet
- Ovitrelle Epar Medicine Overview - enDocument3 pagesOvitrelle Epar Medicine Overview - enPhysics with V SagarNo ratings yet
- PDPHDocument19 pagesPDPHcardiacanesthesiaNo ratings yet
- CMC Vellore Summer Admission Bulletin 2020 Revised 16 Nov 2020Document58 pagesCMC Vellore Summer Admission Bulletin 2020 Revised 16 Nov 2020Allen ChrysoNo ratings yet
- Inpatient Psychiatric Unit Patient HandbookDocument7 pagesInpatient Psychiatric Unit Patient HandbookJuanCarlos Yogi0% (1)
- Petronas Gas PGB PDFDocument34 pagesPetronas Gas PGB PDFAhmad Aiman100% (5)
- Riwayat Pendidikan Riwayat PekerjaanDocument36 pagesRiwayat Pendidikan Riwayat PekerjaanRam PrototokonNo ratings yet
- Aunt Minnie Pediatric NeuroDocument15 pagesAunt Minnie Pediatric NeuroRommel OliverasNo ratings yet
- Minnesota Multiphasic Personality Inventory TestDocument26 pagesMinnesota Multiphasic Personality Inventory TestGicu BelicuNo ratings yet
- Factors Associated With Compassion Satisfaction, Burnout, andDocument30 pagesFactors Associated With Compassion Satisfaction, Burnout, andpratiwi100% (1)
- Bipolar Disorder Symptoms, Causes and TreatmentDocument108 pagesBipolar Disorder Symptoms, Causes and TreatmentMaica LectanaNo ratings yet
- Hexa Health guides patients through surgery processDocument2 pagesHexa Health guides patients through surgery processSarvesh KashyapNo ratings yet
- Incident Reporting and Investigation ProcedureDocument8 pagesIncident Reporting and Investigation ProcedureWitara Saja67% (3)
- Medifocus April 2007Document61 pagesMedifocus April 2007Pushpanjali Crosslay HospitalNo ratings yet
- Shy BookletDocument28 pagesShy BookletDesmond ScottNo ratings yet