You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Pentester BlueprintDocument27 pagesThe Pentester Blueprintjames smith100% (1)
- Differential Pressure Hazards in DivingDocument4 pagesDifferential Pressure Hazards in DivingmrudhulrajNo ratings yet
- API Standard 521 - Guide For Pressure-Relieving and Depressuring Systems PDFDocument9 pagesAPI Standard 521 - Guide For Pressure-Relieving and Depressuring Systems PDFYosmar Guzman100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Asme NM.2-2018Document126 pagesAsme NM.2-2018aneeshjokay75% (4)
- DROPS Recommended Practice 2017Document62 pagesDROPS Recommended Practice 2017TobeFrankNo ratings yet
- Chemicals Zetag DATA Powder Magnafloc 351 - 0410Document2 pagesChemicals Zetag DATA Powder Magnafloc 351 - 0410PromagEnviro.comNo ratings yet
- Summary of Macondo InquiriesDocument20 pagesSummary of Macondo InquiriesmrudhulrajNo ratings yet
- How To Develop A Super MemoryDocument12 pagesHow To Develop A Super Memoryazik zakiNo ratings yet
- Transformer Fire Protection: Facilities Instructions, Standards, and Techniques Volume 3-32Document43 pagesTransformer Fire Protection: Facilities Instructions, Standards, and Techniques Volume 3-32GualaNo ratings yet
- Transformer Fire Protection: Facilities Instructions, Standards, and Techniques Volume 3-32Document43 pagesTransformer Fire Protection: Facilities Instructions, Standards, and Techniques Volume 3-32GualaNo ratings yet
- Heal Yourself in Ten Minutes AJDocument9 pagesHeal Yourself in Ten Minutes AJJason Mangrum100% (1)
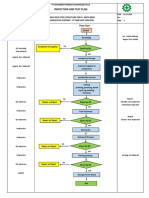
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- JPK-056-07-L-1754 - Rev 0Document245 pagesJPK-056-07-L-1754 - Rev 0aibek100% (1)
- EU MDR FlyerDocument12 pagesEU MDR FlyermrudhulrajNo ratings yet
- D Formation Damage StimCADE FDADocument30 pagesD Formation Damage StimCADE FDAEmmanuel EkwohNo ratings yet
- Case Study: Management Standards For Stress: 11% Improvement in Stress Sickness AbsenceDocument2 pagesCase Study: Management Standards For Stress: 11% Improvement in Stress Sickness AbsencemrudhulrajNo ratings yet
- Science Review 2018Document63 pagesScience Review 2018mrudhulrajNo ratings yet
- Foresight Report: The Human Impact of The Changing Nature of WorkDocument26 pagesForesight Report: The Human Impact of The Changing Nature of WorkmrudhulrajNo ratings yet
- HSE's Science and Evidence Investment Plan: Current PositionDocument3 pagesHSE's Science and Evidence Investment Plan: Current PositionmrudhulrajNo ratings yet
- Science Evidence Strategy 1620Document6 pagesScience Evidence Strategy 1620mrudhulrajNo ratings yet
- Science Review 2020 NewDocument65 pagesScience Review 2020 NewmrudhulrajNo ratings yet
- Science Review 2019Document67 pagesScience Review 2019mrudhulrajNo ratings yet
- Science Review 2017Document56 pagesScience Review 2017mrudhulrajNo ratings yet
- AJ Bell Youinvest AJ Bell Youinvest SIPP Pre-Retirement Pension Fund IllustrationDocument7 pagesAJ Bell Youinvest AJ Bell Youinvest SIPP Pre-Retirement Pension Fund IllustrationmrudhulrajNo ratings yet
- Process Approach To Drinking Water Quality Risk Assessment Using Bowtie AnalysisDocument9 pagesProcess Approach To Drinking Water Quality Risk Assessment Using Bowtie AnalysismrudhulrajNo ratings yet
- HSE Science and Evidence Delivery Plan 2019-2020 Focuses on Regulatory FrameworksDocument23 pagesHSE Science and Evidence Delivery Plan 2019-2020 Focuses on Regulatory FrameworksmrudhulrajNo ratings yet
- Xxiv Paper 26 PDFDocument13 pagesXxiv Paper 26 PDFmrudhulrajNo ratings yet
- Experiences With Fires and ExplosionsDocument10 pagesExperiences With Fires and ExplosionsmrudhulrajNo ratings yet
- Uncertainty in Explosion Risk AssessmentDocument10 pagesUncertainty in Explosion Risk AssessmentmrudhulrajNo ratings yet
- Offshore Release Data - Trends in Underlying Causes: A B A, B A A BDocument12 pagesOffshore Release Data - Trends in Underlying Causes: A B A, B A A BmrudhulrajNo ratings yet
- Offshore Ladders for Escape to Sea GuideDocument7 pagesOffshore Ladders for Escape to Sea GuidemrudhulrajNo ratings yet
- Moving From Tenant To Nuclear Licence Holder On A GB Nuclear Licensed SiteDocument6 pagesMoving From Tenant To Nuclear Licence Holder On A GB Nuclear Licensed SitemrudhulrajNo ratings yet
- COS Accreditation SEMSToolkit FactSheet ForPrintDocument2 pagesCOS Accreditation SEMSToolkit FactSheet ForPrintmrudhulrajNo ratings yet
- A Guide To Gas Detection - White PaperDocument8 pagesA Guide To Gas Detection - White PapermrudhulrajNo ratings yet
- Eu Offshore Safety DirectiveDocument16 pagesEu Offshore Safety DirectivemrudhulrajNo ratings yet
- Ireland Business Visa Application IndiaDocument10 pagesIreland Business Visa Application IndiamrudhulrajNo ratings yet
- KPMG Climate Change Attitude SurveyDocument6 pagesKPMG Climate Change Attitude SurveymrudhulrajNo ratings yet
- Rajasthan PET Chemistry 1997 Exam with Detailed SolutionsDocument34 pagesRajasthan PET Chemistry 1997 Exam with Detailed SolutionsYumit MorwalNo ratings yet
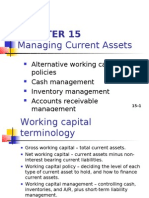
- CHAPTER 15 Managing Current AssetsDocument26 pagesCHAPTER 15 Managing Current AssetsAhsanNo ratings yet
- Volume 1Document168 pagesVolume 1lalitendu jenaNo ratings yet
- Persuasive Essay Eng 101nDocument6 pagesPersuasive Essay Eng 101napi-341545248No ratings yet
- MPQ2908 - 48V Buck Converter Automotive Reference DesignDocument4 pagesMPQ2908 - 48V Buck Converter Automotive Reference DesignShubham KaklijNo ratings yet
- Undas Deployment PadsDocument15 pagesUndas Deployment PadsVic NairaNo ratings yet
- Understanding Anxiety Disorders and Abnormal PsychologyDocument7 pagesUnderstanding Anxiety Disorders and Abnormal PsychologyLeonardo YsaiahNo ratings yet
- Platinum Gazette 29 November 2013Document12 pagesPlatinum Gazette 29 November 2013Anonymous w8NEyXNo ratings yet
- Cswip Visual Welding Inspector 3.0 BrochureDocument1 pageCswip Visual Welding Inspector 3.0 BrochureNasfauzan100% (2)
- Versidrain 150: Green RoofDocument2 pagesVersidrain 150: Green RoofMichael Tiu TorresNo ratings yet
- Byk-A 525 enDocument2 pagesByk-A 525 enさいとはちこNo ratings yet
- Arecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionDocument23 pagesArecaceae or Palmaceae (Palm Family) : Reported By: Kerlyn Kaye I. AsuncionNamae BacalNo ratings yet
- EPF, EPS, Gratuity, Superannuation & Group Life Insurance Nomination FAQsDocument4 pagesEPF, EPS, Gratuity, Superannuation & Group Life Insurance Nomination FAQsHemanth DhananjayNo ratings yet
- 12 2022 Salary Slip SintexDocument1 page12 2022 Salary Slip SintexpathyashisNo ratings yet
- ZP Series Silicon Rectifier: Standard Recovery DiodesDocument1 pageZP Series Silicon Rectifier: Standard Recovery DiodesJocemar ParizziNo ratings yet
- Bandong 3is Q4M6Document6 pagesBandong 3is Q4M6Kento RyuNo ratings yet
- IC 33 Question PaperDocument12 pagesIC 33 Question PaperSushil MehraNo ratings yet
- Bio ViberDocument7 pagesBio ViberMarco BuntNo ratings yet
- IOSA Self Evaluation Form - 31 October 2014Document45 pagesIOSA Self Evaluation Form - 31 October 2014pknight2010No ratings yet
- Mechanical Thrombectomy For Acute Ischemic StrokeDocument19 pagesMechanical Thrombectomy For Acute Ischemic StrokeCarlos Alfredo Vargas QuinteroNo ratings yet
- Catálogo SEDIVERDocument32 pagesCatálogo SEDIVEREnver Rojas DiazNo ratings yet
- Balloons FullDocument19 pagesBalloons FullHoan Doan NgocNo ratings yet