You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Good-Enough Sex Model For Couple Sexual SatisfactionDocument13 pagesThe Good-Enough Sex Model For Couple Sexual SatisfactionwernikNo ratings yet
- Niko Tinbergen and The Red Patch On The Herring Gull's BeakDocument10 pagesNiko Tinbergen and The Red Patch On The Herring Gull's BeakchurianaNo ratings yet
- A Literature Review of The Epidemiology of Sepsis in Latin AmericaDocument9 pagesA Literature Review of The Epidemiology of Sepsis in Latin AmericasmileybutterflyNo ratings yet
- Blood Donation Thesis StatementDocument7 pagesBlood Donation Thesis Statementjessicacannellamanchester100% (2)
- Lecture 8 Colloids Electrokinetic PhenomenonDocument33 pagesLecture 8 Colloids Electrokinetic PhenomenonJunaid Parker0% (1)
- Gynecology PDFDocument537 pagesGynecology PDFCrystal Nguyen100% (1)
- Modul Praktikum Patologi Anatomi Fakultas Kedokteran Universitas Muhammadiyah Palembang Tahun 2015Document23 pagesModul Praktikum Patologi Anatomi Fakultas Kedokteran Universitas Muhammadiyah Palembang Tahun 2015TasyaNo ratings yet
- Biodiversity and Its ConservationDocument30 pagesBiodiversity and Its Conservationjoshivishwanath100% (1)
- IiiiiiDocument8 pagesIiiiiiAyusriwahyuni RambeNo ratings yet
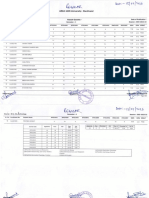
- Result Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Document2 pagesResult Gazette Regular ODD 22 23 1st Semester B.SC Biotechnology. 1Abhishek BhaduriNo ratings yet
- AdatinaDocument1 pageAdatinaCRISTIELI IZABEL FOGUESATTONo ratings yet
- Bacteriological Analytical Manual Chapter 21A Examination of Canned FoodsDocument26 pagesBacteriological Analytical Manual Chapter 21A Examination of Canned FoodsFrancis Dave FloresNo ratings yet
- Dr. John's Mother Tinctures & Dilutions List Dr. John's Mother Tinctures & Dilutions ListDocument6 pagesDr. John's Mother Tinctures & Dilutions List Dr. John's Mother Tinctures & Dilutions ListAnand KumarNo ratings yet
- Lockett Autopsy ReportDocument12 pagesLockett Autopsy ReportNewsOK100% (1)
- Ibiza Medicina 2016 No ChordsDocument260 pagesIbiza Medicina 2016 No ChordsMarilia Lins100% (2)
- Gilliam Autism Rating Scale (GARS-2) : Probability of Autism Is Unlikely, Possibly, Very LikelyDocument3 pagesGilliam Autism Rating Scale (GARS-2) : Probability of Autism Is Unlikely, Possibly, Very LikelyKeishla MojicaNo ratings yet
- Paper Lichen Activity 3Document11 pagesPaper Lichen Activity 3Christopher MoralesNo ratings yet
- Schneider Et Al 2019 Frontiers PL SciDocument18 pagesSchneider Et Al 2019 Frontiers PL SciSaša MarkočevićNo ratings yet
- Womersley Arterial Flow - SimpleDocument10 pagesWomersley Arterial Flow - SimplebhatsindhoorNo ratings yet
- Taurine 3 Cellular and Regulatory MechanismsDocument510 pagesTaurine 3 Cellular and Regulatory MechanismsYoBjjNo ratings yet
- (1227) Validation of Microbial Recovery From Pharmacopeial Articles Usp39Document5 pages(1227) Validation of Microbial Recovery From Pharmacopeial Articles Usp39fadjarNo ratings yet
- Mitosis Internet LessonDocument3 pagesMitosis Internet LessonGLENMAR VINEGASNo ratings yet
- Earl Eugene Castro - Bio 32 Learning Activity 1Document2 pagesEarl Eugene Castro - Bio 32 Learning Activity 1EARL CASTRONo ratings yet
- Emmanuel Acha AsongalemDocument9 pagesEmmanuel Acha AsongalemPaulin NanaNo ratings yet
- PRL 8Document2 pagesPRL 8anna ticaNo ratings yet
- Concentration of Methanol and Ethanol in Alcoholic Drink by GCDocument10 pagesConcentration of Methanol and Ethanol in Alcoholic Drink by GCYunus HidayatNo ratings yet
- Lecture 5: Global-Scale Physical-Biological Interaction ProcessesDocument13 pagesLecture 5: Global-Scale Physical-Biological Interaction ProcessesMaraschino1993No ratings yet
- Principles of Keyline DesignDocument2 pagesPrinciples of Keyline Designinfo1381No ratings yet
- Soma Devi InvoiceDocument1 pageSoma Devi InvoiceManeesh Verma100% (1)
- What Is The Objective of Endurance TrainingDocument5 pagesWhat Is The Objective of Endurance TrainingNaveed WarraichNo ratings yet