You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- PBL 12 - Adrenal GlandsDocument7 pagesPBL 12 - Adrenal GlandsKrishna OochitNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Peds Shelf NotesDocument88 pagesPeds Shelf Notesskeebs23100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PN NCLEX PRACTICE TESTDocument75 pagesPN NCLEX PRACTICE TESTjedisay1100% (1)
- 2020-Biochem-Activity-16 - BIOCHEMISTRY OF HORMONESDocument32 pages2020-Biochem-Activity-16 - BIOCHEMISTRY OF HORMONESGabrielle John HernaezNo ratings yet
- Glucocorticoids and Mineralocorticoids: Roles and EffectsDocument27 pagesGlucocorticoids and Mineralocorticoids: Roles and EffectsAmrit GaireNo ratings yet
- PN NCLEX - Integrated (A)Document63 pagesPN NCLEX - Integrated (A)fairwoods89% (19)
- 18 HypokalemiaDocument54 pages18 HypokalemiaJoel Topf100% (2)
- CEM4719 Noradrenaline v2Document1 pageCEM4719 Noradrenaline v2drpiratheepan4274No ratings yet
- ENDOCRINE SYSTEM - Anatomy and PhysiologyDocument10 pagesENDOCRINE SYSTEM - Anatomy and PhysiologyJay Crishnan Morales CajandingNo ratings yet
- Technical Comparison of On-Line vs. Line-Interactive UPS DesignsDocument14 pagesTechnical Comparison of On-Line vs. Line-Interactive UPS Designsdrpiratheepan4274No ratings yet
- Endocrine Pharmacology OverviewDocument52 pagesEndocrine Pharmacology OverviewNicole Opao100% (4)
- Hans Selye. The General Adaptation SyndromeDocument16 pagesHans Selye. The General Adaptation SyndromeCelso Sánchez Ramírez100% (2)
- Blue Book - Guidelines For The Control of Infectious DiseaseDocument271 pagesBlue Book - Guidelines For The Control of Infectious DiseaseavarathunnyNo ratings yet
- Learning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14Document9 pagesLearning Objectives:: Pathophysiology & Therapeutics, I (MSPR 521) Lecture No. 14adzhangNo ratings yet
- Spirometer Handbook NacaDocument24 pagesSpirometer Handbook NacaebrycNo ratings yet
- Spirometer Handbook NacaDocument24 pagesSpirometer Handbook NacaebrycNo ratings yet
- Adrenal GuidelinesDocument20 pagesAdrenal GuidelinesUtziel Abel Carrillo GonzalezNo ratings yet
- Metabolic Syndrome Diagnosis Guidelines ComparisonDocument4 pagesMetabolic Syndrome Diagnosis Guidelines Comparisondrpiratheepan4274No ratings yet
- PACES - Abdominal MarksheetsDocument2 pagesPACES - Abdominal Marksheetsdrpiratheepan4274No ratings yet
- Adrenal GuidelinesDocument20 pagesAdrenal GuidelinesUtziel Abel Carrillo GonzalezNo ratings yet
- DM in Aids PatientDocument10 pagesDM in Aids Patientdrpiratheepan4274No ratings yet
- Licorice AbuseDocument14 pagesLicorice Abusedrpiratheepan4274No ratings yet
- TFT Guideline Final Version July 2006Document86 pagesTFT Guideline Final Version July 2006Boris Miguel HernándezNo ratings yet
- EndocrinologyDocument60 pagesEndocrinologyrinahn100% (1)
- Insuline Tolerance TestDocument2 pagesInsuline Tolerance Testdrpiratheepan4274No ratings yet
- Australian Doctor Flying and HealthDocument6 pagesAustralian Doctor Flying and Healthdrpiratheepan4274No ratings yet
- Familial Hyperlipidaemia Risk AssessmentDocument7 pagesFamilial Hyperlipidaemia Risk Assessmentdrpiratheepan4274No ratings yet
- LongActingGLP-1RAgonists 2011Document6 pagesLongActingGLP-1RAgonists 2011madelosriosNo ratings yet
- Diagnosis and Treatment of Peripheral Arterial DiseaseDocument5 pagesDiagnosis and Treatment of Peripheral Arterial Diseasedrpiratheepan4274No ratings yet
- DM NewDocument8 pagesDM Newdrpiratheepan4274No ratings yet
- 'S Assessment SeriesDocument22 pages'S Assessment Seriesdrpiratheepan4274No ratings yet
- Gestatational DMDocument65 pagesGestatational DMdrpiratheepan4274No ratings yet
- Intubation Review: SFC HillDocument26 pagesIntubation Review: SFC Hilldrpiratheepan4274No ratings yet
- Central Venous Catheterization: To The EditorDocument3 pagesCentral Venous Catheterization: To The Editordrpiratheepan4274No ratings yet
- Intubacion OrotraquealDocument5 pagesIntubacion OrotraquealEduardo SantosNo ratings yet
- Positive-Pressure Ventilation With A Face Mask and A Bag-Valve DeviceDocument3 pagesPositive-Pressure Ventilation With A Face Mask and A Bag-Valve Devicedrpiratheepan4274No ratings yet
- BUDDHIST ERA 2556 - 2557: Victory Belongs To The Most PerseveringDocument1 pageBUDDHIST ERA 2556 - 2557: Victory Belongs To The Most Perseveringsamitha505No ratings yet
- Adrenaline intravenous infusion calculations guideDocument1 pageAdrenaline intravenous infusion calculations guidedrpiratheepan4274No ratings yet
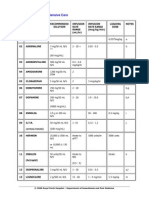
- Drug Infusions For Intensive CareDocument2 pagesDrug Infusions For Intensive CarejaionlyNo ratings yet
- Terpenes and SteroidsDocument38 pagesTerpenes and SteroidsZabrina Tan CuaNo ratings yet
- Functions of The Mineralocorticoids Aldosterone Reg of Ald SecretDocument5 pagesFunctions of The Mineralocorticoids Aldosterone Reg of Ald SecretEstellaNo ratings yet
- Hormonal control of salt and water balance in vertebratesDocument6 pagesHormonal control of salt and water balance in vertebratesFarel RizkiNo ratings yet
- Chapter 6 - Endocrine System 2Document12 pagesChapter 6 - Endocrine System 2AyeshaNo ratings yet
- Return To The Medical Biochemistry PageDocument8 pagesReturn To The Medical Biochemistry Pagevibhav82No ratings yet
- Florinef (Fludrocortisone)Document3 pagesFlorinef (Fludrocortisone)E100% (1)
- GlucocorticoidDocument10 pagesGlucocorticoidRauf KhanNo ratings yet
- Chapter 5 Endocrinology 1Document53 pagesChapter 5 Endocrinology 1Abubakar JallohNo ratings yet
- Quimica de MXDocument800 pagesQuimica de MXkimerax100% (2)
- Osmoregulation in Earthworms ExplainedDocument28 pagesOsmoregulation in Earthworms ExplainedMa-anJaneDiamosNo ratings yet
- DrugsDocument98 pagesDrugsReo PratapNo ratings yet
- Extrarenal Effects of Aldosterone On Potassium HomeostasisDocument8 pagesExtrarenal Effects of Aldosterone On Potassium HomeostasisKhánh Nguyễn NgọcNo ratings yet
- Adrenocorticosteroids: C39 Adrenocorticosteroids & Adrenocortical AntagonistsDocument5 pagesAdrenocorticosteroids: C39 Adrenocorticosteroids & Adrenocortical AntagonistsHydieNo ratings yet
- Immune Regulation by GlucocorticoidsDocument35 pagesImmune Regulation by GlucocorticoidsSyifa SariNo ratings yet
- Review Test Submission - Graded Quiz - Endocrine - Human ..Document9 pagesReview Test Submission - Graded Quiz - Endocrine - Human ..hannahNo ratings yet
- Comprehensive Stress Management 13th Edition Greenberg Test BankDocument45 pagesComprehensive Stress Management 13th Edition Greenberg Test BankJacquelineSinghwoad100% (12)
- Iups Programa 25072017 BXDocument76 pagesIups Programa 25072017 BXSonja BuvinicNo ratings yet
- Mineralocorticoids: Shajeer. SDocument42 pagesMineralocorticoids: Shajeer. SShajeer SalimNo ratings yet
- Corticosteroids: Saitoti S. Clinical Pharmacologist UdomDocument33 pagesCorticosteroids: Saitoti S. Clinical Pharmacologist UdomZabron LuhendeNo ratings yet