You might also like
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementFrom EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementNo ratings yet
- 00 RWISO JOURNAL - Roth Williams International Society of PDFDocument61 pages00 RWISO JOURNAL - Roth Williams International Society of PDFanon_768201406No ratings yet
- Biomechanics of Extra-Alveolar Mini-Implant Use in The Infrazygomatic Crest Area For Asymmetrical Correction of Class II Subdivision MalocclusionDocument9 pagesBiomechanics of Extra-Alveolar Mini-Implant Use in The Infrazygomatic Crest Area For Asymmetrical Correction of Class II Subdivision MalocclusionhabeebNo ratings yet
- An Interview With Chris ChangDocument5 pagesAn Interview With Chris ChangDominikaSkórkaNo ratings yet
- Manual Bio Art 4000sDocument22 pagesManual Bio Art 4000sArchitNo ratings yet
- Seminars in OrthodonticsDocument3 pagesSeminars in Orthodonticsgriffone1No ratings yet
- DV y Plano OclusalDocument8 pagesDV y Plano OclusalDiego Andres Hincapie HerreraNo ratings yet
- Topic - Maxillary Transverse DiscrepancyDocument42 pagesTopic - Maxillary Transverse Discrepancy王鈴鈞No ratings yet
- MARPE AbdAllah BahaaDocument90 pagesMARPE AbdAllah BahaaOmar AbodoniaNo ratings yet
- MSE 10.1016@j.ajodo.2016.10.025Document11 pagesMSE 10.1016@j.ajodo.2016.10.025Neycer Catpo NuncevayNo ratings yet
- EssixDocument5 pagesEssixdent in dentistNo ratings yet
- Mandibular Incisor Extraction TherapyDocument10 pagesMandibular Incisor Extraction TherapyLeonardo LamimNo ratings yet
- Spradley1981 PDFDocument10 pagesSpradley1981 PDFFernando Ruiz BorsiniNo ratings yet
- Van BeekDocument4 pagesVan BeekThendral DevanathanNo ratings yet
- CBCT Imaging To Diagnose and Correct The Failure Ofmaxillary Arch Retraction With IZC Screw Anchorage PDFDocument14 pagesCBCT Imaging To Diagnose and Correct The Failure Ofmaxillary Arch Retraction With IZC Screw Anchorage PDFSoe San KyawNo ratings yet
- 3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFDocument7 pages3D Technologies For Precision in Orthodontics - 2018 - Seminars in Orthodontics PDFOmy J. CruzNo ratings yet
- Ortodoncia Brackets inDocument17 pagesOrtodoncia Brackets injavierNo ratings yet
- Elemento II AndrewsDocument8 pagesElemento II AndrewsdbarrioslambNo ratings yet
- Fixed ApplainceDocument2 pagesFixed ApplainceSaravanan KanagavelNo ratings yet
- Growth Patterns in Subjects With Long and Short FacesDocument12 pagesGrowth Patterns in Subjects With Long and Short FacesMatt SanoudosNo ratings yet
- The Story of The Master and Legend: 2015 American Association of Orthodontists Annual SessionDocument11 pagesThe Story of The Master and Legend: 2015 American Association of Orthodontists Annual SessionPaolaLNo ratings yet
- Spear 2008Document9 pagesSpear 2008IlseNo ratings yet
- MARPE AbdAllah Bahaaa Ref NewDocument23 pagesMARPE AbdAllah Bahaaa Ref NewAya ElsayedNo ratings yet
- Gingiva and Orthodontic Treatment PDFDocument15 pagesGingiva and Orthodontic Treatment PDFmutansNo ratings yet
- Space AnalysisDocument43 pagesSpace AnalysismarieNo ratings yet
- ABO American Board of Orthodontics 2013-CALIBRATION-KITDocument63 pagesABO American Board of Orthodontics 2013-CALIBRATION-KITEryson Thiago PradoNo ratings yet
- Practical and Theoretical Seminar Of: Bioprogressive ScienceDocument5 pagesPractical and Theoretical Seminar Of: Bioprogressive SciencesaberNo ratings yet
- McLaughlin Manual ViewDocument88 pagesMcLaughlin Manual Viewnadia Tovar GarciaNo ratings yet
- Evolution of Treatment Mechanics PDFDocument9 pagesEvolution of Treatment Mechanics PDFJunaid Israr - OrthodonticsNo ratings yet
- Diastema Closure and Long-Term Stability - JCO-OnLINEDocument15 pagesDiastema Closure and Long-Term Stability - JCO-OnLINEAbad SalcedoNo ratings yet
- Wjo 2 3 Kim1 PDFDocument11 pagesWjo 2 3 Kim1 PDFGoutam NookalaNo ratings yet
- Evolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveDocument9 pagesEvolution of Treatment Mechanics and Contemporary Appliance Design in Orthodontics: A 40-Year PerspectiveBeatriz ChilenoNo ratings yet
- Tweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisDocument56 pagesTweed AJO 1946 - The Frankfort Mandibular Plane Angle in Orthodontic Diagnosis, Classification, Treatment Planning and PrognosisAnonymous 1uVifBp6100% (1)
- Steiner Analysis Cecil CDocument6 pagesSteiner Analysis Cecil Cjeff diazNo ratings yet
- KimDocument12 pagesKimIvanna H. A.No ratings yet
- Applicability of Pont's Index in OrthodonticsDocument5 pagesApplicability of Pont's Index in OrthodonticsmelovebeingmeNo ratings yet
- -PeriodontаI InstrumentationDocument459 pages-PeriodontаI InstrumentationDANIELA ALEJANDRA VARGAS SANCHEZNo ratings yet
- Maxillary Molar Distalization With Modified Trans Palatal Arch and Mini Implants PDFDocument6 pagesMaxillary Molar Distalization With Modified Trans Palatal Arch and Mini Implants PDFSoe San KyawNo ratings yet
- Facial Height Index: Case ReportDocument7 pagesFacial Height Index: Case ReportEstefania MontoyaNo ratings yet
- V3 - PLANETS of ORTHODONTICS - Volume III - Biomechanics and Tooth MovementDocument89 pagesV3 - PLANETS of ORTHODONTICS - Volume III - Biomechanics and Tooth MovementPhanQuangHuyNo ratings yet
- J Am Dent Assoc 2009 Spear 1160 6Document8 pagesJ Am Dent Assoc 2009 Spear 1160 6alimordecai945No ratings yet
- MVT Varsitile +Document28 pagesMVT Varsitile +drimtiyaz123No ratings yet
- Bracket Synergy RDocument6 pagesBracket Synergy RDaniel Garcia VergaraNo ratings yet
- Sarver Mission PossibleDocument13 pagesSarver Mission PossibleAndrea Cárdenas Sandoval100% (1)
- Vertical Dimension-Literature ReviewDocument6 pagesVertical Dimension-Literature ReviewAvina BanariNo ratings yet
- Cephalometrics in Clinical Practice: Beverly Hills, CalifDocument22 pagesCephalometrics in Clinical Practice: Beverly Hills, CalifDanilo Jose GomezNo ratings yet
- Spear Kokich 07Document19 pagesSpear Kokich 07Aya Ibrahim Yassin100% (1)
- Extractions in Orthodontics: An UpdateDocument10 pagesExtractions in Orthodontics: An Updatedrzana78100% (1)
- Bolton Analysis According To ABODocument54 pagesBolton Analysis According To ABOkerminkNo ratings yet
- Orthodontic Root Resorption: Abhijeet JaiswalDocument56 pagesOrthodontic Root Resorption: Abhijeet JaiswalDr.Sakshi katyalNo ratings yet
- 3differentiated Orthodontic Mechanics For Dental Midline CorrectionDocument6 pages3differentiated Orthodontic Mechanics For Dental Midline Correctionabad salcedoNo ratings yet
- Tip - EdgeDocument37 pagesTip - EdgearshabharataNo ratings yet
- BoltonDocument26 pagesBoltonDryashpal SinghNo ratings yet
- The Retention Protocol 2017 Seminars in OrthodonticsDocument12 pagesThe Retention Protocol 2017 Seminars in Orthodonticsdruzair007No ratings yet
- Correcting The Class II Subdivision MalocclusionDocument2 pagesCorrecting The Class II Subdivision MalocclusionplsssssNo ratings yet
- The FOA Reference For Fiber Optics - Fiber Optic TestingDocument19 pagesThe FOA Reference For Fiber Optics - Fiber Optic TestingvsalaiselvamNo ratings yet
- Updated G10 Class Routine Effective From 12 January 2023Document1 pageUpdated G10 Class Routine Effective From 12 January 2023NiloyNo ratings yet
- Unit 3Document12 pagesUnit 3Erik PurnandoNo ratings yet
- Dawn of Solar PV CookingDocument5 pagesDawn of Solar PV CookingAbhinav AgrawalNo ratings yet
- Straight LineDocument15 pagesStraight LineAyanNo ratings yet
- 3 Tasks and ANS - Gamma Maths PDFDocument6 pages3 Tasks and ANS - Gamma Maths PDFNora ZhangNo ratings yet
- PEH Q3 Long QuizDocument1 pagePEH Q3 Long QuizBenedict LumagueNo ratings yet
- IV. Network Modeling, Simple SystemDocument16 pagesIV. Network Modeling, Simple SystemJaya BayuNo ratings yet
- 4 Force & ExtensionDocument13 pages4 Force & ExtensionSelwah Hj AkipNo ratings yet
- RACI Matrix Design For Managing Stakeholders in PRDocument12 pagesRACI Matrix Design For Managing Stakeholders in PRRheza Nugraha Prabareswara100% (1)
- World's Standard Model G6A!: Low Signal RelayDocument9 pagesWorld's Standard Model G6A!: Low Signal RelayEgiNo ratings yet
- Arduino Oscilloscope ProjectDocument12 pagesArduino Oscilloscope ProjectSathya Narayan100% (1)
- Ad149 Manual RDocument69 pagesAd149 Manual RCharityNo ratings yet
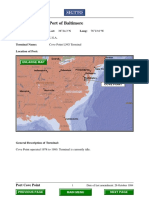
- Port Name: Port of BaltimoreDocument17 pagesPort Name: Port of Baltimoremohd1khairul1anuarNo ratings yet
- S TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpDocument6 pagesS TR GEN ID (Component Marking) (Rev 3 2009) - AN Marked UpsnclgsraoNo ratings yet
- 02-Building Cooling LoadsDocument3 pages02-Building Cooling LoadspratheeshNo ratings yet
- Structural Analysis and Design of Pressure Hulls - The State of The Art and Future TrendsDocument118 pagesStructural Analysis and Design of Pressure Hulls - The State of The Art and Future TrendsRISHABH JAMBHULKARNo ratings yet
- Dual Op Amp and Voltage Reference Ap4310/ADocument12 pagesDual Op Amp and Voltage Reference Ap4310/AМихаил ЯненкоNo ratings yet
- NCP Orif Right Femur Post OpDocument2 pagesNCP Orif Right Femur Post OpCen Janber CabrillosNo ratings yet
- Math AA SL P 1 Marks SchemeDocument6 pagesMath AA SL P 1 Marks SchemeMrin GhoshNo ratings yet
- CheckList For Checking of Drawings-R1Document4 pagesCheckList For Checking of Drawings-R1jatin kalraNo ratings yet
- SP Essay 1Document14 pagesSP Essay 1api-511870420No ratings yet
- MTH100Document3 pagesMTH100Syed Abdul Mussaver ShahNo ratings yet
- AssessmentDocument3 pagesAssessmentpalflaxNo ratings yet
- Worlds Apart: A Story of Three Possible Warmer WorldsDocument1 pageWorlds Apart: A Story of Three Possible Warmer WorldsJuan Jose SossaNo ratings yet
- Market AnalysisDocument4 pagesMarket AnalysisSaniya CharaniyaNo ratings yet
- Bomba MixerDocument2 pagesBomba MixerBinelli79No ratings yet
- AssessmentDocument9 pagesAssessmentJuan Miguel Sapad AlpañoNo ratings yet
- Assignment Booklet July 2021Document22 pagesAssignment Booklet July 2021Saksham TiwariNo ratings yet
- FYP ProposalDocument11 pagesFYP ProposalArslan SamNo ratings yet