You might also like
- PSA Blueprint February2014 PDFDocument20 pagesPSA Blueprint February2014 PDFlauras3005No ratings yet
- Introduction to Clinical Effectiveness and Audit in HealthcareFrom EverandIntroduction to Clinical Effectiveness and Audit in HealthcareNo ratings yet
- Prescribing Safety AssessmentDocument21 pagesPrescribing Safety AssessmentBoussad CHAIBNo ratings yet
- ACTD PartIVClinical Nov05Document50 pagesACTD PartIVClinical Nov05TueNo ratings yet
- PJ ONLINE Pharmacoeconomics 2Document3 pagesPJ ONLINE Pharmacoeconomics 2Anshari StressNo ratings yet
- 2008 2231 20 88Document7 pages2008 2231 20 88maulikpatel2709No ratings yet
- ACTD Rev.1 Part IV Clinical DocumentDocument50 pagesACTD Rev.1 Part IV Clinical DocumentRaeanne SabadoNo ratings yet
- Designing of Formulary:: Step I: Ÿ ŸDocument4 pagesDesigning of Formulary:: Step I: Ÿ ŸbalamuruganNo ratings yet
- What Is A Risk Management PlanDocument2 pagesWhat Is A Risk Management PlanAre Pee EtcNo ratings yet
- Pasquale Esposito Antonio Dal Canton Author Information Article Notes Information Cited byDocument11 pagesPasquale Esposito Antonio Dal Canton Author Information Article Notes Information Cited byshoaib samNo ratings yet
- Tools For Quality MeasurementDocument11 pagesTools For Quality MeasurementFranhel alexandra GarciaNo ratings yet
- TSQM PDFDocument13 pagesTSQM PDFSenandungNacitaNo ratings yet
- Laboratory Medicine Quality IndicatorsDocument14 pagesLaboratory Medicine Quality IndicatorskinnusaraiNo ratings yet
- Desain Study Halaman 31 40Document5 pagesDesain Study Halaman 31 40capita doankNo ratings yet
- 556-Appropriateness of Clinical Decision Support - Final White Paper-Wei WuDocument15 pages556-Appropriateness of Clinical Decision Support - Final White Paper-Wei Wuapi-398506399No ratings yet
- NHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)Document21 pagesNHMRC Evidence Hierarchy Designations of Levels of Evidence' According To Type of Research Question (Including Explanatory Notes)varahamihirNo ratings yet
- Development of The Manchester Framework For The Evaluation of Emergency Department Pharmacy ServicesDocument9 pagesDevelopment of The Manchester Framework For The Evaluation of Emergency Department Pharmacy ServicesalfinadyaNo ratings yet
- CritCare ContentOutlineForPublication20170913Document6 pagesCritCare ContentOutlineForPublication20170913Ali MehdiNo ratings yet
- PharmacotherapyDocument6 pagesPharmacotherapyAli MehdiNo ratings yet
- Chapter 12 Systematic Review of Prognostic TestsDocument13 pagesChapter 12 Systematic Review of Prognostic TestsMuammar EmirNo ratings yet
- 10 - 01 - Investigator BrochureDocument6 pages10 - 01 - Investigator BrochureLaura SaglietiNo ratings yet
- Inappropriate Prescribing: A Systematic Overview of Published Assessment ToolsDocument11 pagesInappropriate Prescribing: A Systematic Overview of Published Assessment ToolsKaraengGalesongNo ratings yet
- 08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyDocument10 pages08 Preventing In-Facility Pressure Ulcers As A Patient Safety StrategyAmanda DavisNo ratings yet
- Applying The Analytic Hierarchy Process in Healthcare Research: A Systematic Literature Review and Evaluation of ReportingDocument27 pagesApplying The Analytic Hierarchy Process in Healthcare Research: A Systematic Literature Review and Evaluation of Reportingnormand67No ratings yet
- T2 - The Nursing Process and PharmacologyDocument7 pagesT2 - The Nursing Process and PharmacologyTRISHA MAE BATAUSANo ratings yet
- Understanding PharmacoeconomicsDocument52 pagesUnderstanding PharmacoeconomicsAlina-Maria CojanNo ratings yet
- Drug Utilisation ReviewDocument33 pagesDrug Utilisation ReviewkeerthanaNo ratings yet
- Drug Utilization Evaluation FinalDocument13 pagesDrug Utilization Evaluation FinalNikkiiNo ratings yet
- Literature Review On Medication Errors in HospitalsDocument7 pagesLiterature Review On Medication Errors in Hospitalsfvgjcq6aNo ratings yet
- 10 - Drug DevelopmentDocument5 pages10 - Drug DevelopmentLaura SaglietiNo ratings yet
- Rational drug use factors and indicatorsDocument14 pagesRational drug use factors and indicatorsSteven A'Baqr EgiliNo ratings yet
- GhiduriDocument20 pagesGhiduriCaraba CorinaNo ratings yet
- Guide To Development of Practice GuidelinesDocument4 pagesGuide To Development of Practice GuidelinesCarlos TobarNo ratings yet
- On the Shelf Life of Pharmaceutical ProductsDocument8 pagesOn the Shelf Life of Pharmaceutical ProductsMihir DixitNo ratings yet
- Pharmacoeconomics As Applied To Hospital Pharmacy HandoutDocument20 pagesPharmacoeconomics As Applied To Hospital Pharmacy HandoutLeylu RepatoNo ratings yet
- KN ClinicalGuidelines2Document2 pagesKN ClinicalGuidelines2Mhmd IrakyNo ratings yet
- 1 Pressure Ulcer Case StudyDocument6 pages1 Pressure Ulcer Case StudyTony MutisyaNo ratings yet
- Gesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Document15 pagesGesundheitswesen Hta Kosten Nutzen Key Principles 2008 0Stavros TheodoridisNo ratings yet
- Pre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesDocument6 pagesPre-And Postoperative Management Techniques. Before and After. Part 1: Medical MorbiditiesMostafa FayadNo ratings yet
- Guidelines On Presenting at Journal ClubDocument6 pagesGuidelines On Presenting at Journal ClubreewenNo ratings yet
- Evidence Based Medication General Guidelines For Clinical Pharmacy PracticeDocument10 pagesEvidence Based Medication General Guidelines For Clinical Pharmacy PracticeMahum SohailNo ratings yet
- Research Methods & Reporting: Consolidated Health Economic Evaluation Reporting Standards (CHEERS) StatementDocument6 pagesResearch Methods & Reporting: Consolidated Health Economic Evaluation Reporting Standards (CHEERS) StatementMuhammadNoorIfansyahNo ratings yet
- Conjoint in HEALTH ResearchDocument17 pagesConjoint in HEALTH ResearchDiana Tan May KimNo ratings yet
- Measuring patient expectancy in clinical trialsDocument10 pagesMeasuring patient expectancy in clinical trialssoylahijadeunvampiroNo ratings yet
- Real-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsDocument5 pagesReal-World Evidence: A Better Life Journey For Pharmas, Payers and PatientsCognizantNo ratings yet
- Drug Utilization ReviewDocument36 pagesDrug Utilization ReviewEdilma VargasNo ratings yet
- Cheers Statement IsporDocument5 pagesCheers Statement IsporKatherine CuéllarNo ratings yet
- 8 Economic EvaluationsDocument38 pages8 Economic EvaluationsDemzy AdeniyiNo ratings yet
- A Systematic Review of Pharmacovigilance Systems in Developing Countries Using The WHO Pharmacovigilance IndicatorsDocument27 pagesA Systematic Review of Pharmacovigilance Systems in Developing Countries Using The WHO Pharmacovigilance Indicators67 Rakesh PatilNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument10 pagesMedical Devices Inspection and Maintenance A Literature ReviewlchirinoscautinhoNo ratings yet
- European Medicines Agency: For Human Use IsDocument44 pagesEuropean Medicines Agency: For Human Use IsashwanNo ratings yet
- Making Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchDocument36 pagesMaking Informed Decisions: Assessing Strengths and Weaknesses of Study Designs and Analytic Methods For Comparative Effectiveness ResearchNational Pharmaceutical CouncilNo ratings yet
- Improve patient care with integrated care pathwaysDocument3 pagesImprove patient care with integrated care pathwaysFitri EmiNo ratings yet
- StepsDocument4 pagesStepsshrikantNo ratings yet
- Adult Medical Surgical AtiDocument4 pagesAdult Medical Surgical Atiapi-243590841No ratings yet
- Module 6-Key Attributes of Cost AnalysesDocument3 pagesModule 6-Key Attributes of Cost AnalysesLou CalderonNo ratings yet
- Assignment InfoDocument4 pagesAssignment Infoabenezer g/kirstosNo ratings yet
- How, in Principle, Should Quality of Care Be Measured?Document4 pagesHow, in Principle, Should Quality of Care Be Measured?Feronika ekaNo ratings yet
- Jay Chou - Coral Sea PDFDocument3 pagesJay Chou - Coral Sea PDFnpganNo ratings yet
- Getting Started With OneDrive PDFDocument1 pageGetting Started With OneDrive PDFmegaNo ratings yet
- Christmas Poster 13v2 PDFDocument1 pageChristmas Poster 13v2 PDFByron Lu MorrellNo ratings yet
- Free Trial 28 FebDocument1 pageFree Trial 28 FebByron Lu Morrell0% (1)
- Reason J. Human ErrorDocument3 pagesReason J. Human ErrorDanielaGarciaNo ratings yet
- ABC Behaviour Chart: Day, Date and Time Antecedent Behaviour Consequence NotesDocument5 pagesABC Behaviour Chart: Day, Date and Time Antecedent Behaviour Consequence NotesByron Lu MorrellNo ratings yet
- Listing LFGSSDocument4 pagesListing LFGSSByron Lu MorrellNo ratings yet
- Beauty And Beast Tab by Kanaho - 飘发 1 - Acoustic Guitar (steel) Songsterr Tabs with Rhythm PDFDocument5 pagesBeauty And Beast Tab by Kanaho - 飘发 1 - Acoustic Guitar (steel) Songsterr Tabs with Rhythm PDFByron Lu MorrellNo ratings yet
- Feedback SheetDocument1 pageFeedback SheetByron Lu MorrellNo ratings yet
- Christmas Poster 13v2Document2 pagesChristmas Poster 13v2Byron Lu MorrellNo ratings yet
- Xray Safety InfoDocument5 pagesXray Safety InfoByron Lu MorrellNo ratings yet
- Christmas Poster 13v2Document1 pageChristmas Poster 13v2Byron Lu MorrellNo ratings yet
- Beauty and Beast Tab by Kanaho - 飘发 1 - Acoustic Guitar (Steel) Songsterr Tabs With RhythmDocument5 pagesBeauty and Beast Tab by Kanaho - 飘发 1 - Acoustic Guitar (Steel) Songsterr Tabs With RhythmByron Lu MorrellNo ratings yet
- The Stanford Prison ExperimentDocument26 pagesThe Stanford Prison ExperimentAsdfac AcsfacNo ratings yet
- Dave Brubeck - Take Five PDFDocument4 pagesDave Brubeck - Take Five PDFBizzled9100% (2)
- S-Type Radio RemovalDocument1 pageS-Type Radio RemovalByron Lu MorrellNo ratings yet
- Twin Links Exchange Programme: Deadline For 2014/15Document10 pagesTwin Links Exchange Programme: Deadline For 2014/15Byron Lu MorrellNo ratings yet
- TicketDocument1 pageTicketByron Lu MorrellNo ratings yet
- Vorl8 030712Document19 pagesVorl8 030712Byron Lu MorrellNo ratings yet
- Accounting Brochure 2013Document20 pagesAccounting Brochure 2013Byron Lu MorrellNo ratings yet
- How To Palpate The AbdomenDocument1 pageHow To Palpate The AbdomenByron Lu MorrellNo ratings yet
- Mainline 1 From 19 MayDocument47 pagesMainline 1 From 19 MayByron Lu MorrellNo ratings yet
- ChrysanthemumFlowerBed JayChouDocument3 pagesChrysanthemumFlowerBed JayChouByron Lu MorrellNo ratings yet
- Condor Geometries 2013 Rev1Document8 pagesCondor Geometries 2013 Rev1Byron Lu MorrellNo ratings yet
- My Heart Will Go On - Tabbed SimplyLuoDocument5 pagesMy Heart Will Go On - Tabbed SimplyLuoNur Farhana Abd RahmanNo ratings yet
- Economics Mark Scehems Unit 6Document23 pagesEconomics Mark Scehems Unit 6Byron Lu MorrellNo ratings yet
- Implanted Seizure Prediction DeviceDocument9 pagesImplanted Seizure Prediction DeviceByron Lu MorrellNo ratings yet
- Cai Hong TabsDocument3 pagesCai Hong TabsByron Lu MorrellNo ratings yet
- 6EC03 Revision Unit 3: Business Economics and Economic Efficiency NotesDocument106 pages6EC03 Revision Unit 3: Business Economics and Economic Efficiency NotesJinaanNo ratings yet
- Department of Conservative Dentistry 2009 FinalDocument160 pagesDepartment of Conservative Dentistry 2009 FinalDr. Nikhil saran67% (3)
- MEDINA - Paz y Ente ReflectionDocument2 pagesMEDINA - Paz y Ente ReflectionMigs MedinaNo ratings yet
- QPMC Liph 2019Document69 pagesQPMC Liph 2019JovelleAnneMondragonNo ratings yet
- Death Obituary Ylrso PDFDocument10 pagesDeath Obituary Ylrso PDFAbbottTerkelsen7No ratings yet
- Unit Kesehatan Sekolah Sehat Jiwa Uks Haji ProgramDocument10 pagesUnit Kesehatan Sekolah Sehat Jiwa Uks Haji ProgramarhanNo ratings yet
- To MS DHQ THQs MIMS Training ScheduleDocument4 pagesTo MS DHQ THQs MIMS Training Schedulesunnykhan bwnNo ratings yet
- DLC BSH Public Report 3.13.2024Document87 pagesDLC BSH Public Report 3.13.2024Boston 25 DeskNo ratings yet
- SENIOR FIRST BROCHURE - Draft v7 - ProductsDocument6 pagesSENIOR FIRST BROCHURE - Draft v7 - ProductsTrinetra AgarwalNo ratings yet
- Assam State Neet-Ug Merit List For Mbbs/Bds Courses, Session-2020Document431 pagesAssam State Neet-Ug Merit List For Mbbs/Bds Courses, Session-2020Asif IqbalNo ratings yet
- Resume Elizabeth WilkinsDocument2 pagesResume Elizabeth Wilkinsapi-301726216No ratings yet
- Foundations - 2 (Part 2)Document54 pagesFoundations - 2 (Part 2)Minatulahamida Al-fitra KadayunanNo ratings yet
- Download ebook Murray Nadels Textbook Of Respiratory Medicine Volumes 1 2 2 Volume Set Pdf full chapter pdfDocument67 pagesDownload ebook Murray Nadels Textbook Of Respiratory Medicine Volumes 1 2 2 Volume Set Pdf full chapter pdfshawn.massey374100% (24)
- Pharma CompanyDocument4 pagesPharma CompanyjennyNo ratings yet
- Department of Pathology Haematology Report:: 7916: Muhammad BakhshDocument1 pageDepartment of Pathology Haematology Report:: 7916: Muhammad BakhshWaseem AkramNo ratings yet
- Inclusion-Exclusion Criteria - SynAct-CS002 BaselineDocument4 pagesInclusion-Exclusion Criteria - SynAct-CS002 Baselineadriana gutanuNo ratings yet
- IAPO Patient Safety Toolkit MainDocument40 pagesIAPO Patient Safety Toolkit MainNeelaj MaityNo ratings yet
- Occupational Therapist Inpatients AHP EDIT VersionDocument12 pagesOccupational Therapist Inpatients AHP EDIT VersionTriciaNo ratings yet
- Opnavinst 6110.1HDocument167 pagesOpnavinst 6110.1HBrandenNo ratings yet
- Medical Records: Making and Retaining Them: What Is A Medical Record?Document6 pagesMedical Records: Making and Retaining Them: What Is A Medical Record?mfadly maulanaNo ratings yet
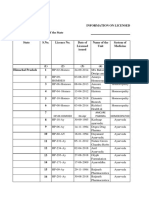
- Himachal Pradesh Aayush ListDocument9 pagesHimachal Pradesh Aayush ListplanetsandtarotNo ratings yet
- Imunisasi Input Jan-JuliDocument79 pagesImunisasi Input Jan-Juliiis muniartiNo ratings yet
- University of The Visayas Philippines: BS BIOLOGY (Pre-Medicine)Document2 pagesUniversity of The Visayas Philippines: BS BIOLOGY (Pre-Medicine)sanjeev kumarNo ratings yet
- Health Care Service Provision under the Universal Health Care Act and Re-devolutionDocument19 pagesHealth Care Service Provision under the Universal Health Care Act and Re-devolutionArabella CatindoyNo ratings yet
- Hubungan Response Time Perawat dan Keberhasilan Penanganan Pasien EmergencyDocument9 pagesHubungan Response Time Perawat dan Keberhasilan Penanganan Pasien Emergencysyaroh fatihatunnisaNo ratings yet
- Member Data Record: Mijares, Sheryl CasimeroDocument1 pageMember Data Record: Mijares, Sheryl CasimeroSheryl MijaresNo ratings yet
- Pulp SensibilityDocument8 pagesPulp SensibilityKarishma SirimullaNo ratings yet
- Alirocumab-75mg Per ML InjectionDocument8 pagesAlirocumab-75mg Per ML InjectionMd. Abdur RahmanNo ratings yet
- Piracetam PDFDocument5 pagesPiracetam PDFAriWahyuNo ratings yet
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- CV Drg. Jeffry KurniawanDocument1 pageCV Drg. Jeffry KurniawanJeffry KurniawanNo ratings yet
- Allen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductFrom EverandAllen Carr's Easy Way to Quit Vaping: Get Free from JUUL, IQOS, Disposables, Tanks or any other Nicotine ProductRating: 5 out of 5 stars5/5 (31)
- Twelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingFrom EverandTwelve Steps and Twelve Traditions: The “Twelve and Twelve” — Essential Alcoholics Anonymous readingRating: 5 out of 5 stars5/5 (11)
- The Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsFrom EverandThe Art of Self-Therapy: How to Grow, Gain Self-Awareness, and Understand Your EmotionsRating: 5 out of 5 stars5/5 (1)
- The Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsFrom EverandThe Heart of Addiction: A New Approach to Understanding and Managing Alcoholism and Other Addictive BehaviorsNo ratings yet
- Stop Drinking Now: The original Easyway methodFrom EverandStop Drinking Now: The original Easyway methodRating: 5 out of 5 stars5/5 (28)
- Alcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousFrom EverandAlcoholics Anonymous, Fourth Edition: The official "Big Book" from Alcoholic AnonymousRating: 5 out of 5 stars5/5 (22)
- Breathing Under Water: Spirituality and the Twelve StepsFrom EverandBreathing Under Water: Spirituality and the Twelve StepsRating: 4.5 out of 5 stars4.5/5 (41)
- The Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingFrom EverandThe Kindness Method: Change Your Habits for Good Using Self-Compassion and UnderstandingRating: 5 out of 5 stars5/5 (10)
- Drunk-ish: A Memoir of Loving and Leaving AlcoholFrom EverandDrunk-ish: A Memoir of Loving and Leaving AlcoholRating: 4 out of 5 stars4/5 (6)
- THE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.From EverandTHE FRUIT YOU’LL NEVER SEE: A memoir about overcoming shame.Rating: 4 out of 5 stars4/5 (7)
- Mommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyFrom EverandMommy Doesn't Drink Here Anymore: Getting Through the First Year of SobrietyRating: 4.5 out of 5 stars4.5/5 (17)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- The Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionFrom EverandThe Stop Drinking Expert: Alcohol Lied to Me Updated And Extended EditionRating: 5 out of 5 stars5/5 (63)
- I Am Enough: From depression, anxiety, and addiction to recoveryFrom EverandI Am Enough: From depression, anxiety, and addiction to recoveryRating: 5 out of 5 stars5/5 (1)
- We Are the Luckiest: The Surprising Magic of a Sober LifeFrom EverandWe Are the Luckiest: The Surprising Magic of a Sober LifeRating: 5 out of 5 stars5/5 (183)
- Easyway Express: Stop Smoking and Quit E-CigarettesFrom EverandEasyway Express: Stop Smoking and Quit E-CigarettesRating: 5 out of 5 stars5/5 (15)
- Recovery – The Sacred Art: The Twelve Steps as Spiritual PracticeFrom EverandRecovery – The Sacred Art: The Twelve Steps as Spiritual PracticeRating: 5 out of 5 stars5/5 (16)
- Sober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholFrom EverandSober Curious: The Blissful Sleep, Greater Focus, Limitless Presence, and Deep Connection Awaiting Us All on the Other Side of AlcoholRating: 4.5 out of 5 stars4.5/5 (127)
- The Language of Letting Go: Daily Meditations on CodependencyFrom EverandThe Language of Letting Go: Daily Meditations on CodependencyRating: 4.5 out of 5 stars4.5/5 (18)
- Clean: Overcoming Addiction and Ending America's Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America's Greatest TragedyRating: 3.5 out of 5 stars3.5/5 (13)
- The Freedom Model for Addictions: Escape the Treatment and Recovery TrapFrom EverandThe Freedom Model for Addictions: Escape the Treatment and Recovery TrapNo ratings yet