You might also like
- How Much Water To Drink When Fasting - Based On The Teachings Of Dr. Eric Berg: Ensuring Proper Water Consumption While FastingFrom EverandHow Much Water To Drink When Fasting - Based On The Teachings Of Dr. Eric Berg: Ensuring Proper Water Consumption While FastingNo ratings yet
- Fluid and Electrolytes JoyDocument10 pagesFluid and Electrolytes JoyM Rizal IsburhanNo ratings yet
- Why Your Body Water Balance Is a Key to Health and Great Shape?From EverandWhy Your Body Water Balance Is a Key to Health and Great Shape?No ratings yet
- Fluid and ElectrolytesDocument10 pagesFluid and ElectrolytesYunisa IrenNo ratings yet
- Fluid and ElectrolytesDocument8 pagesFluid and ElectrolytesCaz SamNo ratings yet
- Supercharging Autophagy - Based On The Teachings Of Dr. Eric Berg: Unleashing Its Full PotentialFrom EverandSupercharging Autophagy - Based On The Teachings Of Dr. Eric Berg: Unleashing Its Full PotentialNo ratings yet
- Maintenance Intravenous Fluid Therapy in Children - UpToDateDocument19 pagesMaintenance Intravenous Fluid Therapy in Children - UpToDaterolland_arrizaNo ratings yet
- The #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandFrom EverandThe #1 Danger Of Prolonged Fasting You Have To Know About - Based On The Teachings Of Dr. Eric Berg: The Most Important Risk To UnderstandNo ratings yet
- Fluids and Electrolytes For PediatricsDocument31 pagesFluids and Electrolytes For PediatricsJeno Luis J. ACUBNo ratings yet
- Metabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentFrom EverandMetabolic Disorders and Critically Ill Patients: From Pathophysiology to TreatmentCarole IchaiNo ratings yet
- Maintenance Fluid Therapy in ChildrenDocument4 pagesMaintenance Fluid Therapy in ChildrenNicole_0No ratings yet
- Author: Section Editor: Deputy EditorDocument11 pagesAuthor: Section Editor: Deputy EditorVictor Lima AraujoNo ratings yet
- F E T C: Luid AND Lectrolyte Herapy IN HildrenDocument12 pagesF E T C: Luid AND Lectrolyte Herapy IN HildrenHartantoRezaGazaliNo ratings yet
- Fluid TherapyDocument27 pagesFluid TherapyRashed ShatnawiNo ratings yet
- The Water Prescription: For Health, Vitality, and RejuvenationFrom EverandThe Water Prescription: For Health, Vitality, and RejuvenationRating: 5 out of 5 stars5/5 (2)
- Dehydration: Body-Fluid CompositionDocument5 pagesDehydration: Body-Fluid CompositionThegreat Mokz Mokz ThegreatNo ratings yet
- Hypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHypercalcemia, (High Blood Calcium) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- 4.fluid and ElectrolytesDocument23 pages4.fluid and ElectrolytesManju KumariNo ratings yet
- Fluid Calculation For Iv InfusionDocument8 pagesFluid Calculation For Iv InfusionAsma SaleemNo ratings yet
- Paed IVFDocument10 pagesPaed IVFnaga tanoojNo ratings yet
- Metabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMetabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Fluids and Electrolytes - PaediatricsDocument52 pagesFluids and Electrolytes - PaediatricsZweNo ratings yet
- Fluid and ElectrolytesDocument137 pagesFluid and ElectrolytesNano Baddour100% (1)
- Fluid and Electrolyte Therapy in NewbornsDocument10 pagesFluid and Electrolyte Therapy in NewbornsJaner BanosNo ratings yet
- Tony - Electrolytes Lect NCMDocument84 pagesTony - Electrolytes Lect NCMJoseph Nawen SindiongNo ratings yet
- Final Report of Importance of WaterDocument5 pagesFinal Report of Importance of WaterTanistha KhandelwalNo ratings yet
- Perioperative Intravenous Fluid Therapy For Adults: Rob Mac Sweeney, Rachel Alexandra Mckendry, Amit BediDocument8 pagesPerioperative Intravenous Fluid Therapy For Adults: Rob Mac Sweeney, Rachel Alexandra Mckendry, Amit BediAnnisa Chaerani BurhanuddinNo ratings yet
- F E T C: Luid and Lectrolyte Herapy in HildrenDocument12 pagesF E T C: Luid and Lectrolyte Herapy in HildrenTania Febria AzizahNo ratings yet
- Fluid and Electrolyte BalanceDocument5 pagesFluid and Electrolyte BalanceBumi Zulheri HermanNo ratings yet
- Test Bank For Lutzs Nutrition and Diet Therapy 7th by MazurDocument15 pagesTest Bank For Lutzs Nutrition and Diet Therapy 7th by Mazurtracywilsonjftmrqknys100% (28)
- Fluid Management For The Pediatric Surgical Patient POWERPOINTDocument34 pagesFluid Management For The Pediatric Surgical Patient POWERPOINTDipta Anggara100% (2)
- Perioperative Fluid ManagementDocument123 pagesPerioperative Fluid ManagementAnonymous 86gki5No ratings yet
- Fluid and Electrolytes.3Document43 pagesFluid and Electrolytes.3Medic PediatruNo ratings yet
- Test Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e MazurDocument16 pagesTest Bank Lutzs Nutrition and Diet Therapy 7th Edition Erin e Mazurjeremiahhartfozxmbqayn100% (11)
- Hipotonicos VS IsotonicosDocument13 pagesHipotonicos VS IsotonicosYeison Duban Gomez CastilloNo ratings yet
- Fluid and Electrolyte Therapy in Newborns PDFDocument7 pagesFluid and Electrolyte Therapy in Newborns PDFdocbinNo ratings yet
- What Is Plasma Osmolality?:, 23 Mei 2007 Fluid and Electrolyte TherapyDocument17 pagesWhat Is Plasma Osmolality?:, 23 Mei 2007 Fluid and Electrolyte TherapyRani ChesarNo ratings yet
- ACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idDocument14 pagesACFrOgCEv6W8PZIOChX2ac TB PsVqkwB2LLEUA - nz2imEUDlJJqTMiew0fEYsQLz7I hoxDAHunIFV - PnnXqTDHrgpAsGRo2r9aPQF4UMBSoquxza - oenQBKFcGXpRcMCDKlMwgjULOtJeC9idCenitserNo ratings yet
- Nursing Fluids and ElectrolytesDocument14 pagesNursing Fluids and Electrolytesaga1028100% (18)
- Fluids SummaryDocument3 pagesFluids Summarymicheal1960No ratings yet
- 10 Fluids and Electrolytes: Cleveland Clinic Intensive Review of Pediatrics, The, 2nd EditionDocument12 pages10 Fluids and Electrolytes: Cleveland Clinic Intensive Review of Pediatrics, The, 2nd EditionaeyousefNo ratings yet
- IV Fluids (What Nurses Need To Know)Document9 pagesIV Fluids (What Nurses Need To Know)ChelseaLovell100% (2)
- Liquidos y Electrolitos 2Document4 pagesLiquidos y Electrolitos 2Jorge MBNo ratings yet
- Dehydration and Rehydration Chapter From The Wilderness Medicine TextbookDocument17 pagesDehydration and Rehydration Chapter From The Wilderness Medicine TextbookcmonBULLSHITNo ratings yet
- Fluid and ElyctrolyteDocument49 pagesFluid and Elyctrolyteuuuhbnb lplhgh100% (2)
- Fluid Electrolyte and AcidBase BalanceDocument33 pagesFluid Electrolyte and AcidBase Balancemoncalshareen3No ratings yet
- Filston 1992Document17 pagesFilston 1992Nilamsari KurniasihNo ratings yet
- Lect 02Document5 pagesLect 02Iptysam Al-AlawiNo ratings yet
- Fluid Electrolytes Bablance 150308Document16 pagesFluid Electrolytes Bablance 150308Shruthi RathishNo ratings yet
- Fluid Replacement GOODocument13 pagesFluid Replacement GOOMansoor TariqNo ratings yet
- Fluid Lec.9Document14 pagesFluid Lec.9ahmed.kald896No ratings yet
- WaterDocument11 pagesWaterAhmed JabbarNo ratings yet
- Perioperative Fluid Management in ChildrenDocument31 pagesPerioperative Fluid Management in ChildrenRashmi SahaNo ratings yet
- Fluid and ElyctrolyteDocument49 pagesFluid and Elyctrolyteuuuhbnb lplhghNo ratings yet
- Kyphosis & LordosisDocument14 pagesKyphosis & LordosisTrixie Marie Sabile Abdulla100% (3)
- Ethical Care 2 Nurs 217Document9 pagesEthical Care 2 Nurs 217api-283946728No ratings yet
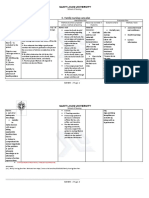
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Breech PresentationDocument27 pagesBreech PresentationNurkamilawati AristaNo ratings yet
- Health Problems MyselfDocument54 pagesHealth Problems MyselfKrishnaveni Murugesh100% (2)
- Tongue Diagnosis in Chinese Medicine (TCM)Document8 pagesTongue Diagnosis in Chinese Medicine (TCM)nepretip50% (2)
- AmysaDocument14 pagesAmysaawanisfauzi90No ratings yet
- Genetic Dis & AnaesthDocument19 pagesGenetic Dis & AnaesthaksinuNo ratings yet
- Asuhan Keperawatan Pada Pasien Dengan Chronic Kidney DiseasesDocument24 pagesAsuhan Keperawatan Pada Pasien Dengan Chronic Kidney DiseasestidaktahudiriNo ratings yet
- Healthcare Statistic in MalaysiaDocument13 pagesHealthcare Statistic in MalaysiaMOZAIDNo ratings yet
- Admission Nursing AssessmentDocument20 pagesAdmission Nursing Assessmentmonir61No ratings yet
- tmpB433 TMPDocument9 pagestmpB433 TMPFrontiersNo ratings yet
- VM in BpocDocument19 pagesVM in BpocAndreea Livia DumitrescuNo ratings yet
- MedStart UMAT Sample and Practice QuestionsDocument55 pagesMedStart UMAT Sample and Practice QuestionsLyn JiangNo ratings yet
- SURESH Testing ProfileDocument3 pagesSURESH Testing Profilefreecharge momNo ratings yet
- The Basal Ganglia and Movement Disorders 2015 RevisedDocument19 pagesThe Basal Ganglia and Movement Disorders 2015 RevisedJoan ChoiNo ratings yet
- Uji Resistensi Antibiotik Terhadap Kultur Bakteri Staphylococcus Aureus PADA RUANG Intensive Care Unit (ICU) RUMAH Sakit Y Kota JambiDocument7 pagesUji Resistensi Antibiotik Terhadap Kultur Bakteri Staphylococcus Aureus PADA RUANG Intensive Care Unit (ICU) RUMAH Sakit Y Kota JambiObrilian Waisman MNo ratings yet
- Observational DescriptiveDocument21 pagesObservational DescriptiveAgus wawaNo ratings yet
- Efektifitas Pelatihan High Alert Medication Terhadap Pengetahuan Dan Sikap Petugas Di RS KIA PKU Muhammadiyah KotagedeDocument4 pagesEfektifitas Pelatihan High Alert Medication Terhadap Pengetahuan Dan Sikap Petugas Di RS KIA PKU Muhammadiyah KotagedeNindy C AbriantyNo ratings yet
- Case StudyDocument2 pagesCase StudyElmer Alberto Lopez PonceNo ratings yet
- KINESIOTHERAPHYDocument40 pagesKINESIOTHERAPHYJeyarajasekar TtrNo ratings yet
- EPC Referral FormDocument1 pageEPC Referral FormCarlos GuerrettaNo ratings yet
- Lithium Use in Pregnancy and The Risk of Cardiac MalformationsDocument10 pagesLithium Use in Pregnancy and The Risk of Cardiac MalformationsRoberto López MataNo ratings yet
- Special - NCLEX - Exam - Jakarta - Students - PDF Filename UTF-8''Special NCLEX Exam - Jakarta StudentsDocument23 pagesSpecial - NCLEX - Exam - Jakarta - Students - PDF Filename UTF-8''Special NCLEX Exam - Jakarta Studentsrizqi100% (1)
- Bag TechniqueDocument23 pagesBag TechniqueMamta Rajput83% (12)
- Insomnia: Management of Underlying ProblemsDocument6 pagesInsomnia: Management of Underlying Problems7OrangesNo ratings yet
- SPC 138523Document4 pagesSPC 138523Pankaj ArgalNo ratings yet
- Texas Has The Highest Maternal Mortality Rate in The Developed WorldDocument5 pagesTexas Has The Highest Maternal Mortality Rate in The Developed WorldDixanetNo ratings yet
- App Ashcraft's Pediatric Surgery 5th EditionDocument8 pagesApp Ashcraft's Pediatric Surgery 5th EditionAndri Feisal NasutionNo ratings yet
- Lomba HHD IgdDocument34 pagesLomba HHD IgdIndra nugrahaNo ratings yet
- Strong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerFrom EverandStrong Is the New Beautiful: Embrace Your Natural Beauty, Eat Clean, and Harness Your PowerRating: 4 out of 5 stars4/5 (5)
- Chair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouFrom EverandChair Yoga: Sit, Stretch, and Strengthen Your Way to a Happier, Healthier YouRating: 3.5 out of 5 stars3.5/5 (5)
- Functional Training and Beyond: Building the Ultimate Superfunctional Body and MindFrom EverandFunctional Training and Beyond: Building the Ultimate Superfunctional Body and MindRating: 4.5 out of 5 stars4.5/5 (1)
- Power of 10: The Once-A-Week Slow Motion Fitness RevolutionFrom EverandPower of 10: The Once-A-Week Slow Motion Fitness RevolutionRating: 3.5 out of 5 stars3.5/5 (11)
- Peak: The New Science of Athletic Performance That is Revolutionizing SportsFrom EverandPeak: The New Science of Athletic Performance That is Revolutionizing SportsRating: 5 out of 5 stars5/5 (96)
- Aging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayFrom EverandAging Backwards: Reverse the Aging Process and Look 10 Years Younger in 30 Minutes a DayNo ratings yet
- Whole Body Barefoot: Transitioning Well to Minimal FootwearFrom EverandWhole Body Barefoot: Transitioning Well to Minimal FootwearRating: 4 out of 5 stars4/5 (16)
- Muscle for Life: Get Lean, Strong, and Healthy at Any Age!From EverandMuscle for Life: Get Lean, Strong, and Healthy at Any Age!Rating: 4.5 out of 5 stars4.5/5 (22)
- Boundless: Upgrade Your Brain, Optimize Your Body & Defy AgingFrom EverandBoundless: Upgrade Your Brain, Optimize Your Body & Defy AgingRating: 4.5 out of 5 stars4.5/5 (66)
- Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandYamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (111)
- Mind Your Body: 4 Weeks to a Leaner, Healthier LifeFrom EverandMind Your Body: 4 Weeks to a Leaner, Healthier LifeRating: 4.5 out of 5 stars4.5/5 (5)
- The Yogi Code: Seven Universal Laws of Infinite SuccessFrom EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessRating: 4.5 out of 5 stars4.5/5 (104)
- Relentless: From Good to Great to UnstoppableFrom EverandRelentless: From Good to Great to UnstoppableRating: 5 out of 5 stars5/5 (784)
- Buteyko Breathing Course Manual: For use with the Advanced Buteyko CourseFrom EverandButeyko Breathing Course Manual: For use with the Advanced Buteyko CourseRating: 5 out of 5 stars5/5 (1)
- Easy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportFrom EverandEasy Strength: How to Get a Lot Stronger Than Your Competition-And Dominate in Your SportRating: 4.5 out of 5 stars4.5/5 (17)
- 80/20 Running: Run Stronger and Race Faster by Training SlowerFrom Everand80/20 Running: Run Stronger and Race Faster by Training SlowerRating: 4.5 out of 5 stars4.5/5 (97)
- Music For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicFrom EverandMusic For Healing: With Nature Sounds For Natural Healing Powers: Sounds Of Nature, Deep Sleep Music, Meditation, Relaxation, Healing MusicRating: 5 out of 5 stars5/5 (1)
- Wall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesFrom EverandWall Pilates: Quick-and-Simple to Lose Weight and Stay Healthy. A 30-Day Journey with + 100 ExercisesNo ratings yet
- The Yoga Sutras of Patanjali: The Final Guide for the Study and Practice of Patanjali's Yoga SutrasFrom EverandThe Yoga Sutras of Patanjali: The Final Guide for the Study and Practice of Patanjali's Yoga SutrasNo ratings yet
- Weight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantFrom EverandWeight Lifting Is a Waste of Time: So Is Cardio, and There’s a Better Way to Have the Body You WantRating: 4.5 out of 5 stars4.5/5 (38)
- If You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsFrom EverandIf You Like Exercise … Chances Are You’Re Doing It Wrong: Proper Strength Training for Maximum ResultsRating: 4.5 out of 5 stars4.5/5 (7)
- Endure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceFrom EverandEndure: Mind, Body, and the Curiously Elastic Limits of Human PerformanceRating: 4.5 out of 5 stars4.5/5 (237)
- Structural Integration and Energy Medicine: A Handbook of Advanced BodyworkFrom EverandStructural Integration and Energy Medicine: A Handbook of Advanced BodyworkRating: 4 out of 5 stars4/5 (1)
- Not a Diet Book: Take Control. Gain Confidence. Change Your Life.From EverandNot a Diet Book: Take Control. Gain Confidence. Change Your Life.Rating: 4.5 out of 5 stars4.5/5 (124)
- Fascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)From EverandFascial Training: With Easy Exercises To More Mobility And Less Pain (10 Minutes Fascia Workout For Home)Rating: 5 out of 5 stars5/5 (3)
- The Yamas & Niyamas: Exploring Yoga's Ethical PracticeFrom EverandThe Yamas & Niyamas: Exploring Yoga's Ethical PracticeRating: 4.5 out of 5 stars4.5/5 (19)