You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Scra 2014Document3 pagesScra 2014Czara DyNo ratings yet
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDocument1 pageMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyNo ratings yet
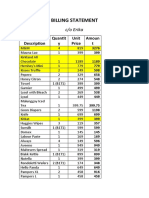
- S&R - Billing StatementDocument4 pagesS&R - Billing StatementCzara DyNo ratings yet
- Castillo vs. RepublicDocument2 pagesCastillo vs. RepublicCzara DyNo ratings yet
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyNo ratings yet
- Banking Mon 7718Document2 pagesBanking Mon 7718Czara DyNo ratings yet
- Corpo Notes 2018 PrelimsDocument14 pagesCorpo Notes 2018 PrelimsCzara DyNo ratings yet
- Institution of Heirs. It Will Not Result To IntestacyDocument9 pagesInstitution of Heirs. It Will Not Result To IntestacyCzara DyNo ratings yet
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyNo ratings yet
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyNo ratings yet
- Sunio v. NLRCDocument3 pagesSunio v. NLRCCzara DyNo ratings yet
- Nil Cases FinalsDocument37 pagesNil Cases FinalsCzara DyNo ratings yet
- TORTS Page 2 Cases SyllabusDocument77 pagesTORTS Page 2 Cases SyllabusCzara DyNo ratings yet
- Annum From July 1, 2013 Until Full PaymentDocument1 pageAnnum From July 1, 2013 Until Full PaymentCzara DyNo ratings yet
- Jimenez vs. FranciscoDocument1 pageJimenez vs. FranciscoCzara DyNo ratings yet
- Q&A Wills Dean AligadaDocument5 pagesQ&A Wills Dean AligadaCzara DyNo ratings yet
- PNB Vs CA DigestDocument3 pagesPNB Vs CA DigestCzara DyNo ratings yet
- Reynolds v. Ca (Dy)Document2 pagesReynolds v. Ca (Dy)Czara DyNo ratings yet
- Memorandum On Charter Change: Presidential Federal ConstitutionDocument1 pageMemorandum On Charter Change: Presidential Federal ConstitutionCzara DyNo ratings yet
- Carpio CalaycayDocument4 pagesCarpio CalaycayCzara DyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chandy C. John - Advances in The Diagnosis and Treatment of Pediatric Infectious Diseases - 2013Document212 pagesChandy C. John - Advances in The Diagnosis and Treatment of Pediatric Infectious Diseases - 2013Alla AlkateebNo ratings yet
- Prostaglandins in Pregnancy: Scott W. Walsh, PHDDocument21 pagesProstaglandins in Pregnancy: Scott W. Walsh, PHDIrene AtimNo ratings yet
- Case Study Endometrial PDFDocument17 pagesCase Study Endometrial PDFapi-279886264No ratings yet
- Chronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLDocument35 pagesChronic Limb Ischaemia: MR Hanif Hussein Consultant Vascular Surgeon, HKLZulzaire ZulkefliNo ratings yet
- Health Grade10 4th QuarterDocument40 pagesHealth Grade10 4th QuarterYnjel HilarioNo ratings yet
- Veterinary Pharmacology 2011Document35 pagesVeterinary Pharmacology 2011Satnam singhNo ratings yet
- Test Bank For Health Psychology 7th Edition TaylorDocument21 pagesTest Bank For Health Psychology 7th Edition Taylorwoodwardpunction2vq46zNo ratings yet
- Trauma in Early Childhood: A Neglected PopulationDocument20 pagesTrauma in Early Childhood: A Neglected PopulationFrancisca AldunateNo ratings yet
- Insulin: For Use On The IMMULITE and Immulite 1000 SystemsDocument27 pagesInsulin: For Use On The IMMULITE and Immulite 1000 SystemsnanikhaNo ratings yet
- Medical Terms and Definitons Commonly Used in MCNDocument15 pagesMedical Terms and Definitons Commonly Used in MCNjoemel gregoriNo ratings yet
- Diabetic Kidney DiseaseDocument69 pagesDiabetic Kidney DiseaseLavina JainNo ratings yet
- Summer PromoDocument1 pageSummer PromobarilesNo ratings yet
- .Au Files Dysbiosis ScoreDocument2 pages.Au Files Dysbiosis ScorekenetmartinNo ratings yet
- Polysomnography (PSG) : Patient Information Patient InformationDocument12 pagesPolysomnography (PSG) : Patient Information Patient Informationhotland sitorusNo ratings yet
- Clinical Experience With MEBO in Treating Paederus DermatitisDocument2 pagesClinical Experience With MEBO in Treating Paederus Dermatitissoumalya481No ratings yet
- Part2MICRO (COMPILED)Document9 pagesPart2MICRO (COMPILED)Thea GonzalesNo ratings yet
- Giles Set CDocument45 pagesGiles Set CPrinting CoNo ratings yet
- 3M Bair Hugger Gown SystemDocument4 pages3M Bair Hugger Gown SystemmochkurniawanNo ratings yet
- Pearls ToxocologicDocument3 pagesPearls ToxocologichsbacongaNo ratings yet
- Slide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Document27 pagesSlide Materi Dr. Kevin Triangto, SPKFR - Heart Failure - PMR4GP 2022Maulia Wisda Era ChresiaNo ratings yet
- Hemotology ReviewDocument61 pagesHemotology ReviewSukma EffendyNo ratings yet
- The Relationship Between Sport and Health: Mentally Physically EmotionalDocument2 pagesThe Relationship Between Sport and Health: Mentally Physically EmotionalNur Aishah Sazali100% (1)
- Cells in The PBSDocument31 pagesCells in The PBSDelzell Dame CasaneNo ratings yet
- Acute Kidney InjuryDocument49 pagesAcute Kidney InjuryfikasywNo ratings yet
- 13 - Digestive System - FullDocument29 pages13 - Digestive System - FullSamson Lee Yun ShenNo ratings yet
- Motor Neurone Disease: J GormallyDocument14 pagesMotor Neurone Disease: J GormallyBambang SutrisnoNo ratings yet
- PPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieDocument98 pagesPPT-"Services and Benefits For Gulf War Veterans" - Anthony HardieAnthony Hardie100% (5)
- Hepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseDocument12 pagesHepatology Research - 2023 - Yoshiji - Management of Cirrhotic Ascites Seven Step Treatment Protocol Based On The JapaneseSarah FaziraNo ratings yet
- Malabsorption SyndromeDocument7 pagesMalabsorption SyndromeHassan.shehri100% (4)
- Human Papillomavirus InfectionDocument78 pagesHuman Papillomavirus InfectionJoaquín PeñaNo ratings yet