You might also like
- برومترك أمراض الكلىDocument36 pagesبرومترك أمراض الكلىTariq Zayan100% (4)
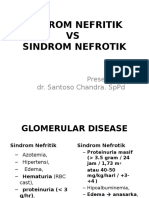
- Glomerular Disease: Acute Nephritic Syndrome Nephrotic Syndrome Chronic GlomerulonephritisDocument18 pagesGlomerular Disease: Acute Nephritic Syndrome Nephrotic Syndrome Chronic GlomerulonephritisironNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument22 pagesSindroma Nefrotik Vs NefritikAyueka EkaNo ratings yet
- Glomerulonephritis-1 (Dr. Soffa)Document58 pagesGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriNo ratings yet
- Practical Hemostasis and ThrombosisFrom EverandPractical Hemostasis and ThrombosisNigel S. KeyNo ratings yet
- Viteri2018 Prevalensi 5Document17 pagesViteri2018 Prevalensi 5adrian revoNo ratings yet
- Glomerular Diseases: DR Rashmi NazarethDocument49 pagesGlomerular Diseases: DR Rashmi NazarethRohit RajeevanNo ratings yet
- Glomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimDocument53 pagesGlomerulonefritis Akut Dan Kronis: DR - Hasan Basri, Sppd-Kgh-FinasimnadddNo ratings yet
- Final CC EdemaDocument31 pagesFinal CC EdematabatchNo ratings yet
- Approach To Patient With Diseases of The Kidney and Urinary Tract FINALDocument9 pagesApproach To Patient With Diseases of The Kidney and Urinary Tract FINALgelskNo ratings yet
- Glomerular DiseaseDocument18 pagesGlomerular DiseaseironNo ratings yet
- Approach To HematuriaDocument45 pagesApproach To HematuriaArun GeorgeNo ratings yet
- Acute Nephritis SyndromeDocument39 pagesAcute Nephritis SyndromeamlymarsNo ratings yet
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- Clinical Approach To RPRF PDFDocument6 pagesClinical Approach To RPRF PDFshankarNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikBobby Fildian Siswanto100% (3)
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritiksiayuNo ratings yet
- Nephrology MRCP1Document174 pagesNephrology MRCP1Raouf Ra'fat Soliman100% (3)
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- Acute Glomerulonephritis: BY: Joice Leokuna Epriwanto Siburian Rina Oktaria Section CDocument12 pagesAcute Glomerulonephritis: BY: Joice Leokuna Epriwanto Siburian Rina Oktaria Section CRiina OktariaNo ratings yet
- C370 Lecture 2 Lecture Notes Part 2Document45 pagesC370 Lecture 2 Lecture Notes Part 2Yan Mui ChanNo ratings yet
- Nephritic Syndrome - Armando HasudunganDocument14 pagesNephritic Syndrome - Armando HasudunganzahraaNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikUswatun Aortatika KhasanahNo ratings yet
- Nephrotic Syndrome-1Document21 pagesNephrotic Syndrome-1Wondimu EliasNo ratings yet
- Nephritic & NephroticDocument18 pagesNephritic & Nephroticlolla2009No ratings yet
- Glomerulonephritis 2Document56 pagesGlomerulonephritis 2Mans FansNo ratings yet
- Sindroma Nefrotik Vs NefritikDocument23 pagesSindroma Nefrotik Vs NefritikBetha456100% (1)
- Acute Glomerulonephritis-Post Streptoccocal GN: MBCHB ViDocument31 pagesAcute Glomerulonephritis-Post Streptoccocal GN: MBCHB ViENOCK BENDERENo ratings yet
- GlomerulonephritisDocument21 pagesGlomerulonephritisDiyoIsworoTunggalKurniawaNo ratings yet
- Post PregnantDocument27 pagesPost PregnantShreyas RavishankarNo ratings yet
- HEMATURIA AND GlomerulonephritisDocument29 pagesHEMATURIA AND GlomerulonephritisSnIP StandredNo ratings yet
- Clinical Approach To: Rapid Progressive GlomerulonephritisDocument38 pagesClinical Approach To: Rapid Progressive GlomerulonephritisMiri PravdaNo ratings yet
- Acute GlomerulonephritisDocument4 pagesAcute GlomerulonephritisJulliza Joy PandiNo ratings yet
- Journal Club Presentation RPGN-1Document53 pagesJournal Club Presentation RPGN-1sagor9364No ratings yet
- Sindroma NefrotikDocument57 pagesSindroma NefrotikAstria Puspita SariNo ratings yet
- Glomerulonephrit Is and Nephrotic SyndromeDocument7 pagesGlomerulonephrit Is and Nephrotic SyndromeJannyNo ratings yet
- Acute GlomeruloNephritis - AGNDocument36 pagesAcute GlomeruloNephritis - AGNKalai VendanNo ratings yet
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 pagesLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanNo ratings yet
- 00 NephrologyDocument98 pages00 Nephrologyeryxsp0% (1)
- APSGNDocument7 pagesAPSGNAvneelNo ratings yet
- +acute GlomerulonephritisDocument19 pages+acute GlomerulonephritisDr. SAMNo ratings yet
- 5 GNAPS EnglishDocument21 pages5 GNAPS Englishdr.Dewi ShintaherNo ratings yet
- Nephrotic SyndromeDocument17 pagesNephrotic SyndromeCitra Wulandari SofyanNo ratings yet
- Dr. YeshwiniDocument34 pagesDr. YeshwiniSai RakshikaNo ratings yet
- AGN and NSDocument2 pagesAGN and NSNur Liyana Ahmad ZakiNo ratings yet
- Approach To Hematuria 2020Document34 pagesApproach To Hematuria 2020Sai RakshikaNo ratings yet
- What Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inDocument6 pagesWhat Is Acute Glomerulonephritis?: Acute Glomerulonephritis (GN) Comprises A Specific Set of Renal Diseases inAnnapoorna SHNo ratings yet
- F Kuliah-Nephritic Syndrome-FK UiSUDocument40 pagesF Kuliah-Nephritic Syndrome-FK UiSUandreNo ratings yet
- 22.AKI ProtocolDocument2 pages22.AKI ProtocolRed DevilNo ratings yet
- 10 Primary Glumerulopathies III - GKDocument2 pages10 Primary Glumerulopathies III - GKGerarld Immanuel KairupanNo ratings yet
- Renal Support in Hepatic Patient: by Mohammed Dabbour Lecturer of Anesthesia Ain Shams UniversityDocument36 pagesRenal Support in Hepatic Patient: by Mohammed Dabbour Lecturer of Anesthesia Ain Shams UniversityTrishenth FonsekaNo ratings yet
- HematuriaDocument42 pagesHematuriaAhmad SobihNo ratings yet
- GLOMERULONEPHRITIS (Bright's Disease)Document8 pagesGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JNo ratings yet
- Lecture (5) - RPGN - CKDDocument20 pagesLecture (5) - RPGN - CKDpoojabappanna25No ratings yet
- Fast Facts: Deficit di piruvato chinasi: Per una maggiore sensibilizzazione su questa rara malattia geneticaFrom EverandFast Facts: Deficit di piruvato chinasi: Per una maggiore sensibilizzazione su questa rara malattia geneticaNo ratings yet
- Fast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareFrom EverandFast Facts: Déficit en pyruvate kinase: Sensibilisation à cette maladie génétique rareRating: 4 out of 5 stars4/5 (1)
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- Ob-Gyn Post Graduate Interns May-June 2017-2018Document1 pageOb-Gyn Post Graduate Interns May-June 2017-2018Marco Paulo Reyes NaoeNo ratings yet
- Williams Endocrinology Large CoverDocument1 pageWilliams Endocrinology Large CoverMarco Paulo Reyes Naoe33% (9)
- Fever and HyperthermiaDocument6 pagesFever and HyperthermiaMarco Paulo Reyes NaoeNo ratings yet
- Assessment of Back Pain-BMJDocument30 pagesAssessment of Back Pain-BMJMarco Paulo Reyes NaoeNo ratings yet
- Table of Contents Williams Endocrinology 13th EditionDocument4 pagesTable of Contents Williams Endocrinology 13th EditionMarco Paulo Reyes NaoeNo ratings yet
- Case Protocol SampleDocument1 pageCase Protocol SampleMarco Paulo Reyes NaoeNo ratings yet
- Pharma Super TableDocument56 pagesPharma Super TableMarco Paulo Reyes NaoeNo ratings yet
- Special Awards - ListDocument7 pagesSpecial Awards - ListMarco Paulo Reyes NaoeNo ratings yet
- Medicine CPC ScriptDocument4 pagesMedicine CPC ScriptMarco Paulo Reyes NaoeNo ratings yet
- APRIL 2017: Aurora Hill and Engineer's Hill Health CentersDocument2 pagesAPRIL 2017: Aurora Hill and Engineer's Hill Health CentersMarco Paulo Reyes NaoeNo ratings yet
- Gastroenterology-Liver, Pancreas and Gall Bladder LecturesDocument7 pagesGastroenterology-Liver, Pancreas and Gall Bladder LecturesMarco Paulo Reyes NaoeNo ratings yet
- Florist ContractDocument1 pageFlorist ContractMarco Paulo Reyes NaoeNo ratings yet
- Medicine Palliative CareDocument5 pagesMedicine Palliative CareMarco Paulo Reyes NaoeNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- Selective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RDocument38 pagesSelective Serotonin Reuptake Inhibitors: Naoe, Marco Paulo RMarco Paulo Reyes NaoeNo ratings yet
- 3rd and 4th Stage of LaborDocument8 pages3rd and 4th Stage of LaborMarco Paulo Reyes NaoeNo ratings yet
- Adrenal Glands: I. Historical BackgroundDocument7 pagesAdrenal Glands: I. Historical BackgroundMarco Paulo Reyes NaoeNo ratings yet
- Diseases of The Muscle - MEDISINA 2017Document9 pagesDiseases of The Muscle - MEDISINA 2017Marco Paulo Reyes NaoeNo ratings yet
- OME Video DurationsDocument7 pagesOME Video DurationsLucas RiosNo ratings yet
- Paediatric Nephrology Syllabus FinalDocument13 pagesPaediatric Nephrology Syllabus FinalClever BarbieNo ratings yet
- Ways To Improve Chronic Kidney Disease OutcomesDocument4 pagesWays To Improve Chronic Kidney Disease OutcomesCharles HermosoNo ratings yet
- Acute Renal Failure: Presented by Peter Fumo, MD, FACPDocument20 pagesAcute Renal Failure: Presented by Peter Fumo, MD, FACPlagathurcNo ratings yet
- Proteinuria and Chronic Kidney DiseaseDocument34 pagesProteinuria and Chronic Kidney DiseaseВалерий ГаврилуцаNo ratings yet
- Biomarkers in Progressive Chronic Kidney Disease. Still A Long Way To GoDocument13 pagesBiomarkers in Progressive Chronic Kidney Disease. Still A Long Way To GoconstanzanazarethNo ratings yet
- KDOQI Clinical Practice Guideline Hemodialysis Update - Public Review Draft FINAL - 20150204 PDFDocument78 pagesKDOQI Clinical Practice Guideline Hemodialysis Update - Public Review Draft FINAL - 20150204 PDFศักดิ์ชัย พูนศรีเจริญกุลNo ratings yet
- Pharmacoeconomic Evaluation of Hemodialysis Patients: A Study of Cost of IllnessDocument6 pagesPharmacoeconomic Evaluation of Hemodialysis Patients: A Study of Cost of IllnessKhairannisa TrisnaNo ratings yet
- Peritoneal Dialysis in Children: Keia Sanderson, Joshua Zaritsky and Bradley A. WaradyDocument20 pagesPeritoneal Dialysis in Children: Keia Sanderson, Joshua Zaritsky and Bradley A. WaradyNi Ketut sugiatiNo ratings yet
- Ultrasound of KidneyDocument5 pagesUltrasound of KidneyMamunNo ratings yet
- AKI in ChildrenDocument43 pagesAKI in ChildrenYonas AwgichewNo ratings yet
- Case Presentation On CKDDocument13 pagesCase Presentation On CKDCalingalan Hussin Caluang100% (1)
- DGEHS Empanelled Hospital-June - 2022Document74 pagesDGEHS Empanelled Hospital-June - 2022Parveen SinghaniaNo ratings yet
- CV Summary 2010Document4 pagesCV Summary 2010ahmad alwaznaNo ratings yet
- Renal Notes Step 2ckDocument34 pagesRenal Notes Step 2cksamreen100% (1)
- Acute Kidney InjuryDocument3 pagesAcute Kidney InjuryHarkirat AtwalNo ratings yet
- Akt RenalDocument4 pagesAkt Renaldzidek7No ratings yet
- Hospital List District WiseDocument34 pagesHospital List District WiseArki100% (1)
- Chronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseDocument23 pagesChronic Renal Failure: Lecture Speaker Dr. V. Lakshmi Prasanna MariseManjunath ArunachalamNo ratings yet
- Ate GlendaDocument3 pagesAte GlendaRomel Ricafort John DavidNo ratings yet
- Hypertension Core CurriculumDocument288 pagesHypertension Core CurriculumJoel Topf100% (1)
- Renal Pathology Unit ExamDocument50 pagesRenal Pathology Unit ExamCherry RahimaNo ratings yet
- Ijnrd 8 125Document13 pagesIjnrd 8 125Muhammad Halil GibranNo ratings yet
- Judgment Sheet in The Islamabad High Court Islamabad: Aamer Farooq JDocument9 pagesJudgment Sheet in The Islamabad High Court Islamabad: Aamer Farooq JAnonymous ar9TCdHNYtNo ratings yet
- NxStage Neph Driver Survey - 18MAR2019 - ProgrammingDocument26 pagesNxStage Neph Driver Survey - 18MAR2019 - ProgrammingKapil BajajNo ratings yet
- Jay Fernando-Gaspar: Ms. Emilia P. Monicimpo, MD, MPH, CseeDocument2 pagesJay Fernando-Gaspar: Ms. Emilia P. Monicimpo, MD, MPH, CseeGaspar De RosaNo ratings yet
- JurnalDocument10 pagesJurnalekalapaleloNo ratings yet
- 1610-Article Text-2547-1-10-20220421Document5 pages1610-Article Text-2547-1-10-20220421Fajar JarrNo ratings yet